

Factors associated with physician-reported treatment status of patients with osteoarthritis pain
- PMID: 35619074
- PMCID: PMC9134575
- DOI: 10.1186/s12891-022-05414-6
Factors associated with physician-reported treatment status of patients with osteoarthritis pain
Abstract
Background: Osteoarthritis (OA) is typically associated with pain, but many patients are not treated.
Methods: This point in time study explored factors associated with treatment status, using logistic regression of data from the Adelphi OA Disease Specific Programme conducted in the United States. Patients' treatment status was based on physician-reported, current: 1) prescription medication for OA vs. none; and 2) physician treatment (prescription medication and/or recommendation for specified nonpharmacologic treatment for OA [physical or occupational therapy, acupuncture, transcutaneous electrical nerve stimulation, or cognitive behavior therapy/psychotherapy]) vs. self-management (no prescription medication or specified nonpharmacologic treatment).
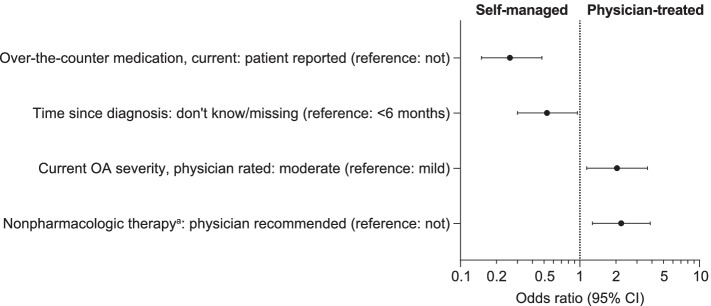
Results: The 841 patients (including 57.0% knee OA, 31.9% hip OA) reported mild (45.4%) or moderate or severe (54.6%) average pain intensity over the last week. The majority were prescribed medication and/or recommended specified nonpharmacologic treatment; 218 were not prescription-medicated and 122 were self-managed. Bivariate analyses showed less severe patient-reported pain intensity and physician-rated OA severity, fewer joints affected by OA, lower proportion of joints affected by knee OA, better health status, lower body mass index, and lower ratings for cardiovascular and gastrointestinal risks, for those not prescribed medication (vs. prescription-medicated). Multivariate analyses confirmed factors significantly (p < 0.05) associated with prescription medication included (odds ratio): physician-rated current moderate OA severity (vs. mild, 2.03), patient-reported moderate OA severity 6 months ago (vs. mild, 1.71), knee OA (vs. not, 1.81), physician-recommended (0.28) and patient-reported (0.43) over-the-counter medication use (vs. not), prior surgery for OA (vs. not, 0.37); uncertain income was also significant. Factors significantly (p < 0.05) associated with physician treatment included (odds ratio): physician-recommended nonpharmacologic therapy requiring no/minimal medical supervision (vs. not, 2.21), physician-rated current moderate OA severity (vs. mild, 2.04), patient-reported over-the-counter medication use (vs. not, 0.26); uncertain time since diagnosis was also significant. Patient-reported pain intensity and most demographic factors were not significant in either model.
Conclusions: Approximately 1 in 4 patients were not prescribed medication and 1 in 7 were self-managed, although many were using over-the-counter medications or nonpharmacologic therapies requiring no/minimal medical supervision. Multiple factors were significantly associated with treatment status, including OA severity and over-the-counter medication, but not pain intensity or most demographics.
Keywords: Osteoarthritis; Pain; Prescription analgesic medication; Real-world clinical practice.
© 2022. The Author(s).
Conflict of interest statement
TJS reports clinical research study support (Pfizer, Lilly, Regeneron, Galapagos, Taiwan Liposome Corporation, Anika Therapeutics) and fees for consultancy/advisory boards (Pfizer, Lilly, GSK, AstraZeneca, Galapagos, Merck). RLR and LV are employees and stockholders of Eli Lilly and Company. JJ, MB, SB, and CW are employees of Adelphi Real World, which received funding from Pfizer and Eli Lilly and Company to conduct the study. LT, AGB, and JCC are employees of Pfizer with stock and/or stock options.
Figures

References
-
- Osteoarthritis Research Society International. White paper: osteoarthritis: a serious disease. Submitted to the U.S. Food and Drug Administration December 1, 2016. Available from: https://www.oarsi.org/sites/default/files/docs/2016/oarsi_white_paper_oa.... Accessed 1 Sept 2020.
-
- Geenen R, Overman CL, Christensen R, Asenlof P, Capela S, Huisinga KL, et al. EULAR recommendations for the health professional's approach to pain management in inflammatory arthritis and osteoarthritis. Ann Rheum Dis. 2018;77:797–807. - PubMed
-
- Nalamachu SR, Robinson RL, Viktrup L, Cappelleri JC, Bushmakin AG, Tive L, et al. Multimodal treatment patterns for osteoarthritis and their relationship to patient-reported pain severity: a cross-sectional survey in the United States. J Pain Res. 2020;13:3415–3425. doi: 10.2147/JPR.S285124. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
