

Tolerance of a Vascularized Composite Allograft Achieved in MHC Class-I-mismatch Swine via Mixed Chimerism
- PMID: 35619720
- PMCID: PMC9128064
- DOI: 10.3389/fimmu.2022.829406
Tolerance of a Vascularized Composite Allograft Achieved in MHC Class-I-mismatch Swine via Mixed Chimerism
Abstract
Background: Vascularized composite allografts (VCAs) allow reconstruction of devastating injuries and amputations, yet require lifelong immunosuppression that is associated with significant morbidity. Induction of immune tolerance of VCAs would permit widespread use of these procedures. VCAs are acquired from deceased donors most likely to be fully-MHC-mismatched (in contrast to living-related renal transplant donor-recipient pairs matched at one MHC haplotype). After achieving VCA tolerance in a swine model equivalent to clinical living-related renal transplants (single-haplotype MHC mismatches: e.g., "mother-daughter"/haploidentical), we tested our protocol in MHC class I, class II, and fully-MHC-mismatched pairs. Although class II mismatched swine demonstrated similar results as the haploidentical scenario (stable mixed chimerism and tolerance), our protocol failed to prevent rejection of class I and full mismatch VCAs. Here, we describe a new adapted conditioning protocol that successfully achieved tolerance across MHC class-I-mismatch barriers in swine.
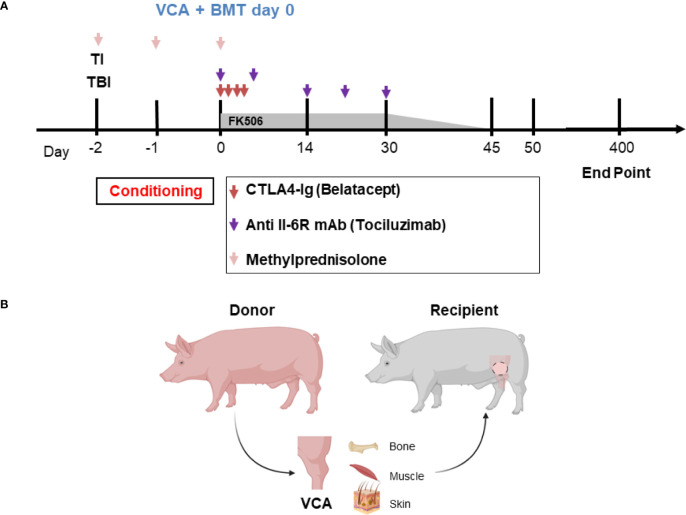
Methods: Swine were treated with non-myeloablative total body and thymic irradiation two days prior to infusion of bone marrow cells from an MHC class I-mismatched donor. They also received a short-term treatment with CTLA4-Ig (Belatacept®) and anti-IL6R mAb (Tociluzimab®) and were transplanted with an osteomyocutaneous VCA from the same donor.
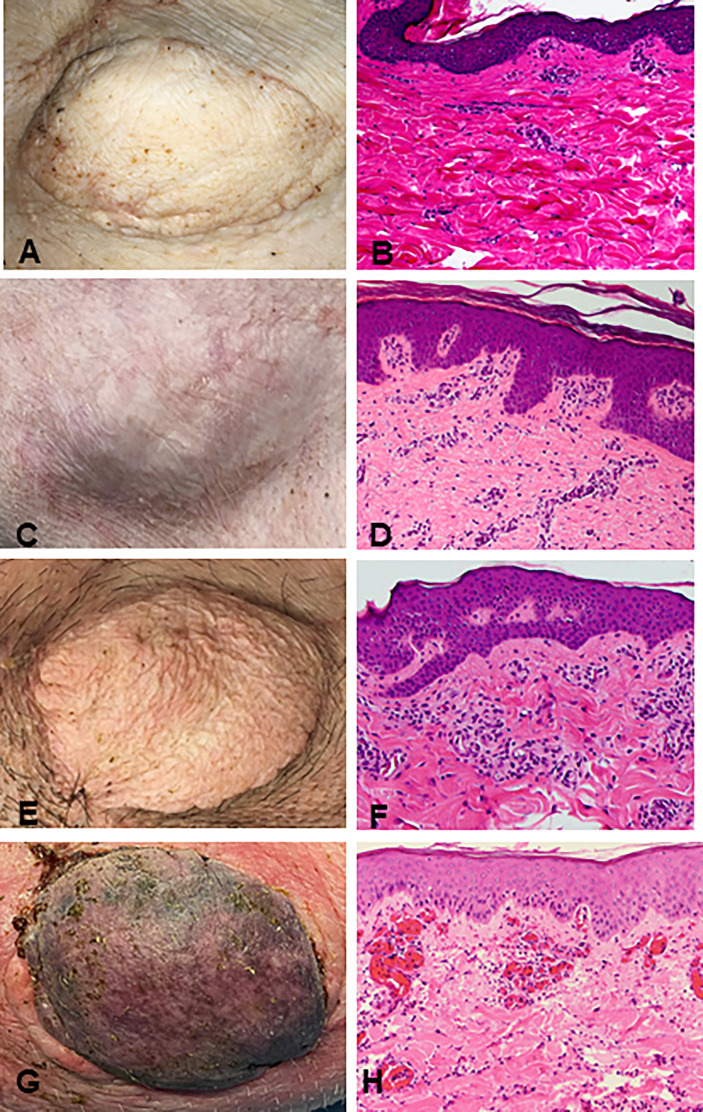
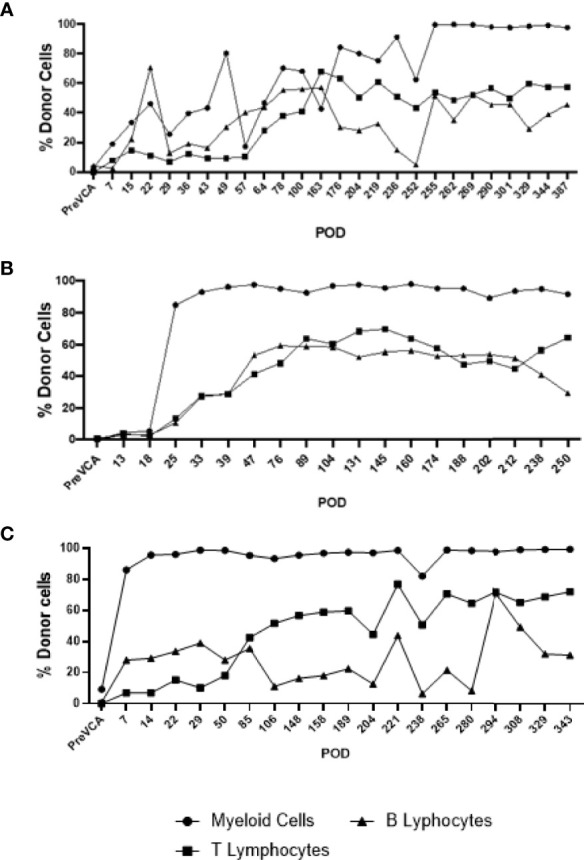
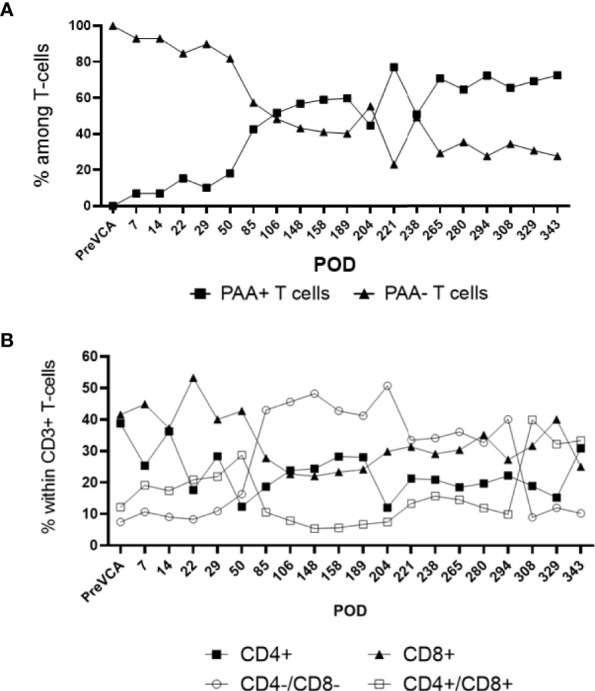
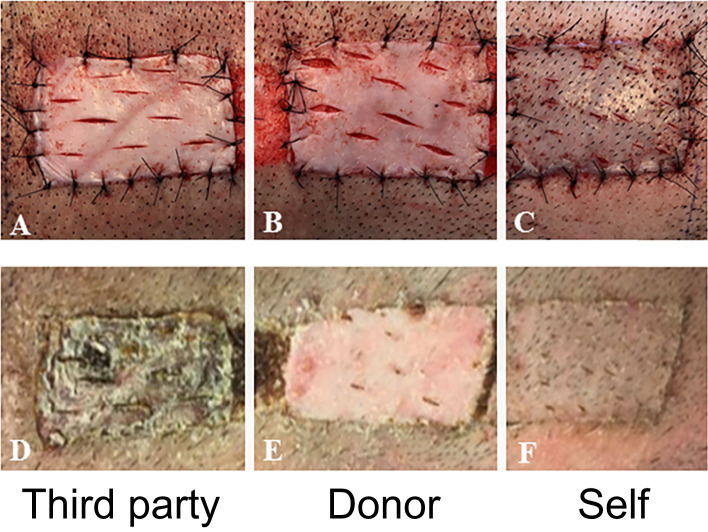
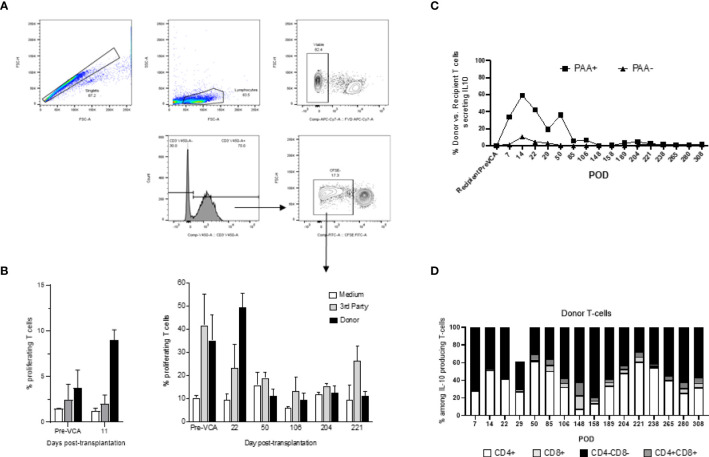
Results: Stable mixed chimerism and tolerance of MHC class-I-mismatched VCAs was achieved in 3 recipients. Allograft tolerance was associated with a sustained lack of anti-donor T cell response and a concomitant expansion of double negative CD4-CD8- T cells producing IL-10.
Conclusions: This study demonstrates the first successful mixed chimerism-induced VCA tolerance in a large animal model across a MHC class-I-mismatch. Future studies aimed at fully-mismatched donor-recipient pairs are under investigation with this protocol.
Keywords: MHC class I; Vascularized composite allotransplantation (VCA); bone marrow transplantation; co-stimulatory blockade; mixed chimerism; skin tolerance.
Copyright © 2022 Lellouch, Andrews, Saviane, Ng, Schol, Goutard, Gama, Rosales, Colvin, Lantieri, Randolph, Benichou and Cetrulo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Petruzzo P, Sardu C, Lanzetta M, Dubernard JM. Report, (2017) of the International Registry on Hand and Composite Tissue Allotransplantation (IRHCTT). Curr Transplant Rep (2017) 4:294–303. doi: 10.1007/s40472-017-0168-3 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials