

Three-hundred and sixty degrees of surgical approaches to the maxillary sinus
- PMID: 35619930
- PMCID: PMC9126161
- DOI: 10.1002/wjo2.12
Three-hundred and sixty degrees of surgical approaches to the maxillary sinus
Abstract
Objectives: To demonstrate three-hundred and sixty degrees of maxillary sinus (MS) surgical approaches using cadaveric dissections, highlighting the step-by-step anatomy of each procedure.
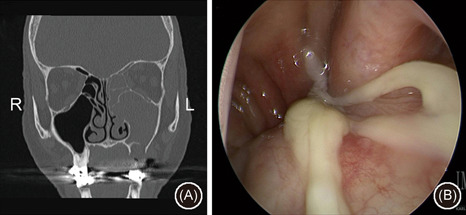
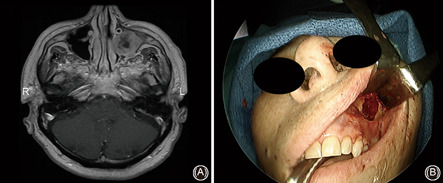
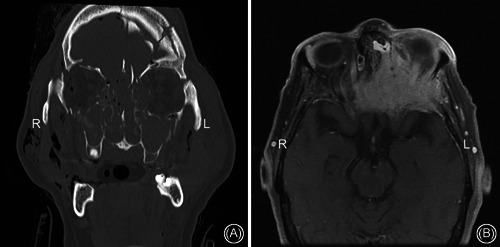
Methods: Two latex-injected cadaveric specimens were utilized to perform surgical dissections to demonstrate different approaches to the MS. The procedures were documented with macroscopic images and endoscopic pictures.
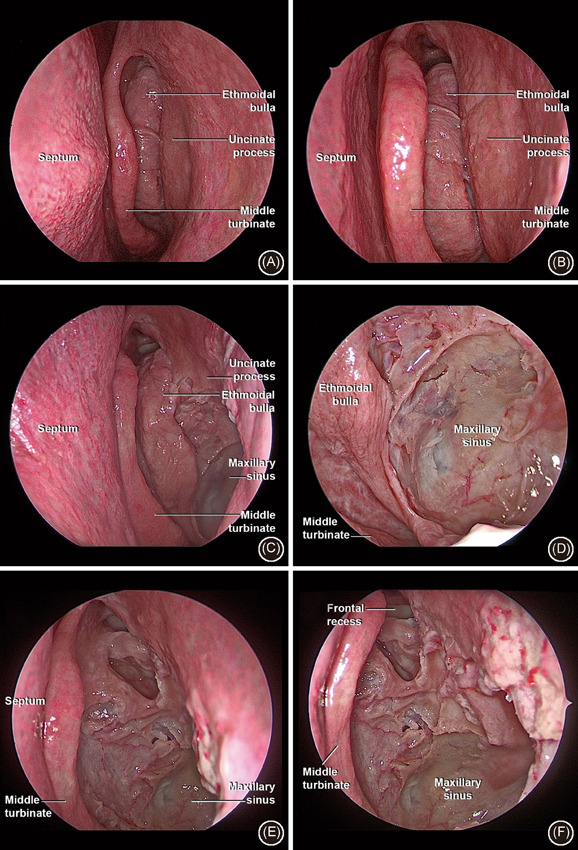
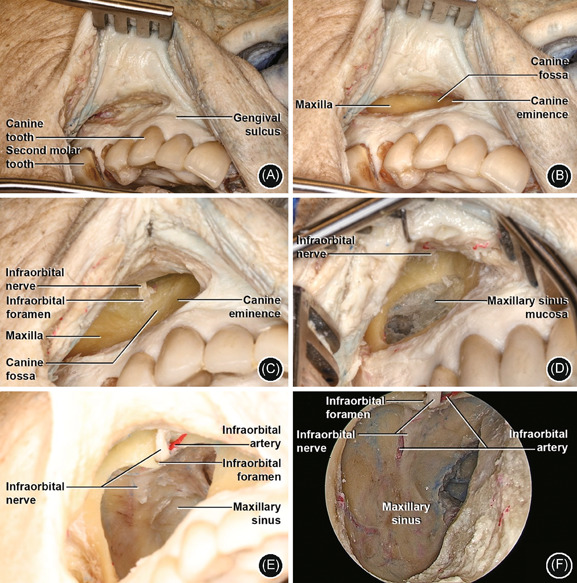
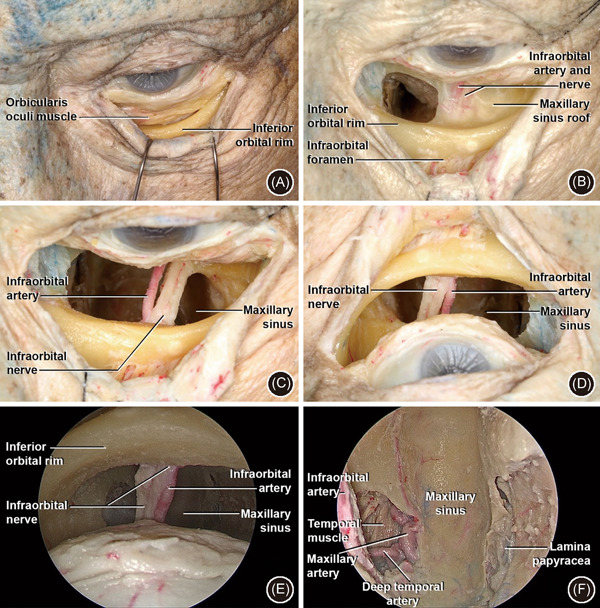
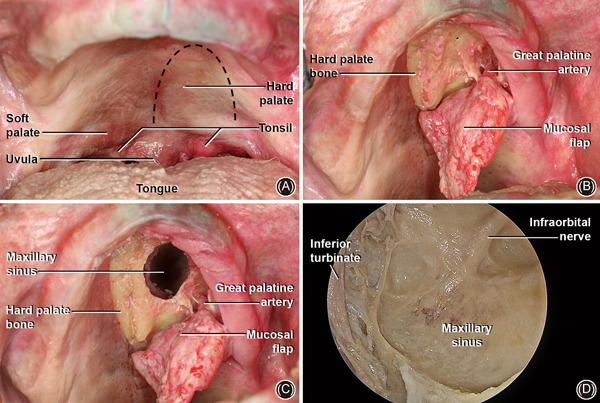
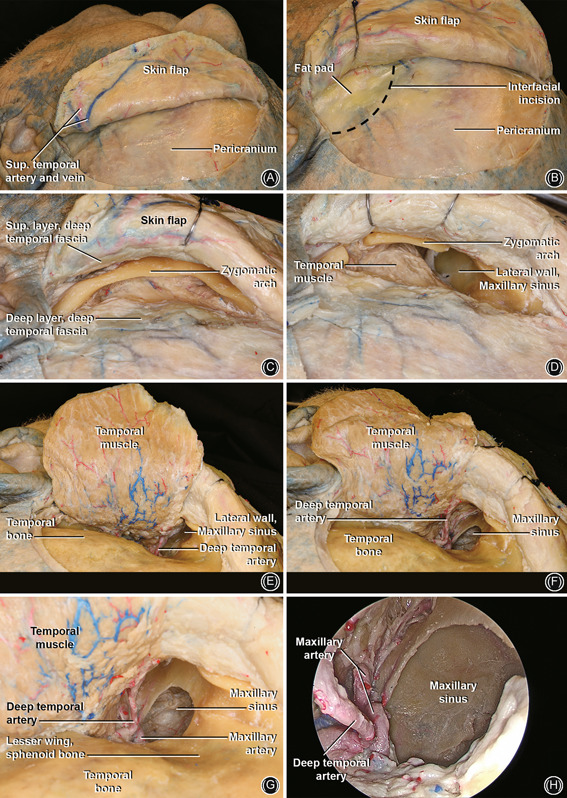
Results: Dissections were performed to approach the MS medially (endoscopic maxillary antrostomy and ethmoidectomy), anteriorly (Caldwell-Luc), superiorly (transconjunctival/transorbital approach), inferiorly (transpalatal approach), and posterolaterally (preauricular hemicoronal approach).
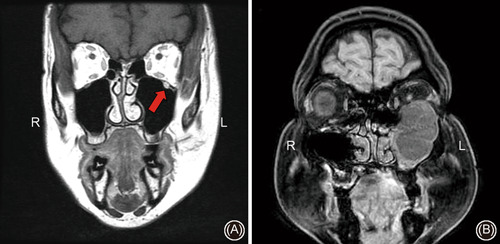
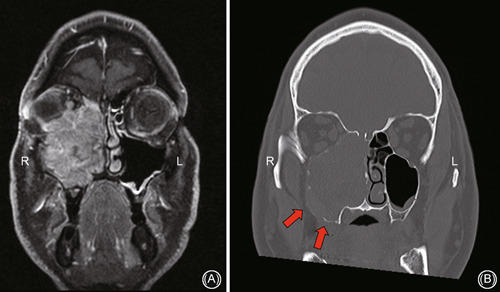
Conclusion: A number of approaches have been described to address pathology in the MS. Surgeons should be familiar with indications, limitations, and surgical anatomy from different perspectives to approach the MS. This paper illustrates anatomic approaches to the MS with detailed step-by-step cadaveric dissections and case examples.
Keywords: Caldwell–Luc; anatomy; dissection; endoscopic sinus surgery; infratemporal fossa; maxillary sinus; pterygopalatine fossa.
© 2022 The Authors. World Journal of Otorhinolaryngology ‐ Head and Neck Surgery published by John Wiley & Sons Ltd on behalf of Chinese Medical Association.
Conflict of interest statement
The authors declare that there are no conflict of interests.
Figures
References
-
- Cho DY, Hwang PH. Results of endoscopic maxillary mega‐antrostomy in recalcitrant maxillary sinusitis. Am J Rhinol. 2008;22:658‐662. - PubMed
-
- Woo HJ, Hwang PH, Kaplan MJ, Choby G. Clinical characteristics and prognostic factors of malignant tumors involving pterygopalatine fossa. Head Neck. 2020;42:281‐288. - PubMed
-
- Wang EW, Gullung JL, Schlosser RJ. Modified endoscopic medial maxillectomy for recalcitrant chronic maxillary sinusitis. Int Forum Allergy Rhinol. 2011;1:493‐497. - PubMed
-
- Peng R, Thamboo A, Choby G, Ma Y, Zhou B, Hwang PH. Outcomes of sinonasal inverted papilloma resection by surgical approach: an updated systematic review and meta‐analysis. Int Forum Allergy Rhinol. 2019;9:573‐581. - PubMed
Publication types
LinkOut - more resources
Full Text Sources