

Impact of extracorporeal CPR with transcatheter heart pump support (ECPELLA) on improvement of short-term survival and neurological outcome in patients with refractory cardiac arrest - A single-site retrospective cohort study
- PMID: 35620182
- PMCID: PMC9127400
- DOI: 10.1016/j.resplu.2022.100244
Impact of extracorporeal CPR with transcatheter heart pump support (ECPELLA) on improvement of short-term survival and neurological outcome in patients with refractory cardiac arrest - A single-site retrospective cohort study
Abstract
Aim: Extracorporeal cardiopulmonary resuscitation (E-CPR) using veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is a novel lifesaving method for refractory cardiac arrest. Although VA-ECMO preserves end-organ perfusion, it may affect left ventricular (LV) recovery due to increased LV load. An emerging treatment modality, ECPELLA, which combines VA-ECMO and a transcatheter heart pump, Impella, can simultaneously provide circulatory support and LV unloading. In this single-site cohort study, we assessed impact of ECPELLA support on clinical outcomes of refractory cardiac arrest patients.
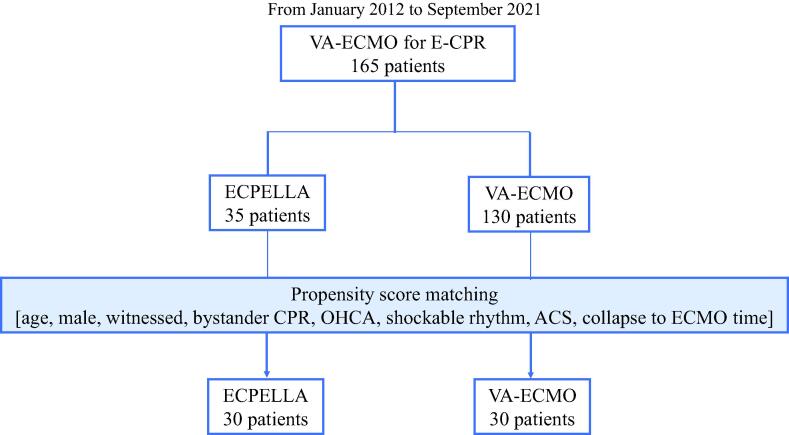
Method: We retrospectively reviewed 165 consecutive cardiac arrest patients, who underwent E-CPR by VA-ECMO with or without intra-aortic balloon pump (IABP) or ECPELLA from January 2012 to September 2021. We assessed 30-day survival rate, neurological outcome, hemodynamic data, and safety profiles including hemolysis, acute kidney injury, blood transfusion and embolic cerebral infarction.
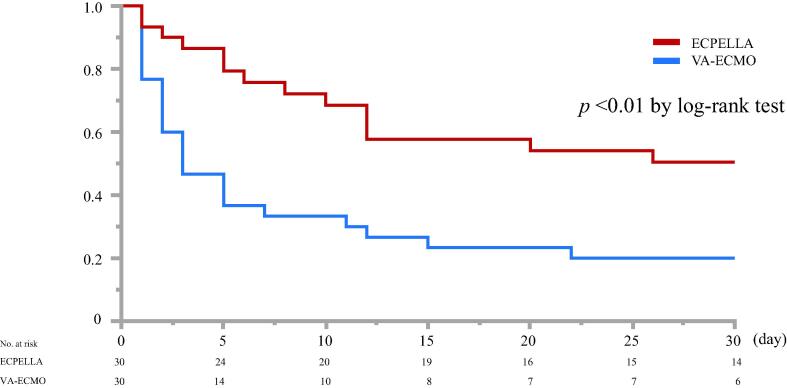
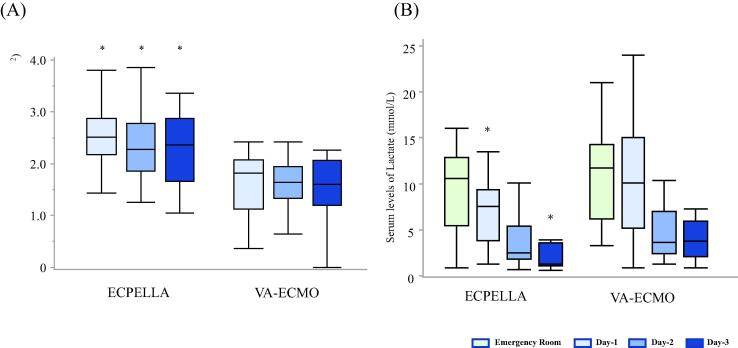
Results: Among 165 E-CPR patients, 35 patients were supported by ECPELLA, and 130 patients were supported by conventional VA-ECMO with or without IABP. Following propensity score matching of 30 ECPELLA and 30 VA-ECMO patients, the 30-day survival (ECPELLA: 53%, VA-ECMO: 20%, p < 0.01) and favorable neurological outcome determined by the Cerebral Performance Category score 1 or 2 (ECPELLA: 33%, VA-ECMO: 7%, p < 0.01) were significantly higher with ECPELLA. Patients receiving ECPELLA also showed significantly higher total mechanical circulatory support flow and lower arterial pulse pressure for the first 3 days (p < 0.01) of treatment. There were no statistical differences in safety profiles between treatment groups.
Conclusion: ECPELLA may be associated with improved 30-day survival and neurological outcome in patients with refractory cardiac arrest.
Keywords: ANOVA, Analysis of variance; CI, Confidential interval; CPC, Cerebral Performance Categories; CPR, Cardiopulmonary resuscitation; CVP, Central venous pressure; Cardiac arrest; Circulatory support; E-CPR, Extracorporeal cardiopulmonary resuscitation; ECPELLA, Combination of VA-ECMO and Impella transcatheter heart pump support; Extracorporeal cardiopulmonary resuscitation; IABP, Intra-aortic balloon pump; Impella; LV unloading; LV, Left ventricle; MCS, Mechanical circulatory support; Myocardial protection; OHCA, Out-of-hospital cardiac arrest; PAPI, Pulmonary artery pulsatility index; VA-ECMO, Venoarterial extracorporeal membrane oxygenation; VIS, Vasoactive inotrope score.
© 2022 The Author(s).
Figures
References
-
- Panchal A.R., Berg K.M., Hirsch K.G., Kudenchuk P.J., del Rios M., Cabanãs J.G., et al. 2019 American Heart Association Focused Update on Advanced Cardiovascular Life Support: Use of Advanced Airways, Vasopressors, and Extracorporeal Cardiopulmonary Resuscitation during Cardiac Arrest: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2019;140(24):e881–e894. doi: 10.1161/CIR.0000000000000732. - DOI - PubMed
-
- Matsuyama T., Irisawa T., Yamada T., Hayakawa K., Yoshiya K., Noguchi K., et al. Impact of Low-Flow Duration on Favorable Neurological Outcomes of Extracorporeal Cardiopulmonary Resuscitation After Out-of-Hospital Cardiac Arrest. Circulation. 2020;141(12):1031–1033. doi: 10.1161/CIRCULATIONAHA.119.044285. - DOI - PubMed
LinkOut - more resources
Full Text Sources
