

Utilizing a Prefabricated Antibiotic-Impregnated Articular Spacer Combined With an Intramedullary Device for Significant Femoral Bone Loss in Periprosthetic Hip Infection
- PMID: 35620353
- PMCID: PMC9126833
- DOI: 10.1016/j.artd.2022.03.013
Utilizing a Prefabricated Antibiotic-Impregnated Articular Spacer Combined With an Intramedullary Device for Significant Femoral Bone Loss in Periprosthetic Hip Infection
Abstract
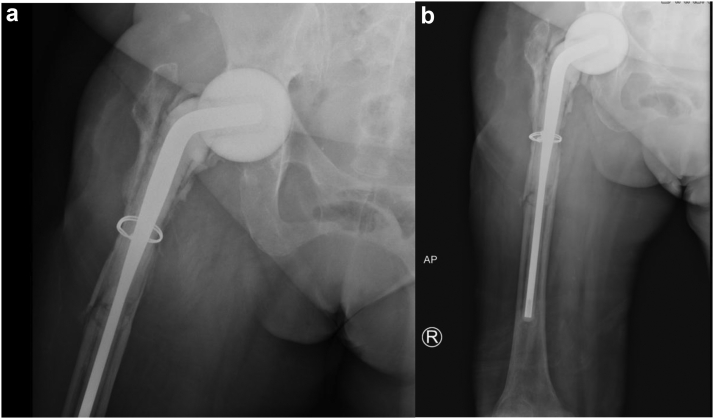
Periprosthetic joint infection can be a devastating complication following total hip arthroplasty, which often requires a lengthy treatment course that is fraught with complications. There are various types of antibiotic-impregnated spacers that can be used to treat periprosthetic hip infections, with articulating spacers being utilized frequently with the goal of preserving patient range of motion and functionality. Many of these articulating spacers have pre-set sizes and stem options, which accommodate the majority of patients. However, when significant femoral bone loss is evident at the time of revision surgery, many articulating spacer options are not sufficient to provide stability, and custom modifications of available spacer constructs may be needed to fill the bony void. The goal of this article is to report a surgical technique that can be used in the salvage of failed antibiotic-impregnated spacers where severe femoral bone loss is present.
Keywords: Infection; PJI; Revision; THA.
© 2022 Published by Elsevier Inc. on behalf of The American Association of Hip and Knee Surgeons.
Figures



References
-
- Lieberman J.R., Callaway G.H., Salvati E.A., Pellicci P.M., Brause B.D. Treatment of the infected total hip arthroplasty with a two-stage reimplantation protocol. Clin Orthop. 1994;301:205–212. - PubMed
-
- Toulson C., Walcott-Sapp S., Hur J., et al. Treatment of infected total hip arthroplasty with a 2-stage reimplantation protocol: update on “our institution’s” experience from 1989 to 2003. J Arthroplasty. 2009;24:1051–1060. - PubMed
-
- Fehring T.K., Odum S., Calton T.F., Mason J.B. Articulating versus static spacers in revision total knee arthroplasty for sepsis. The Ranawat Award. Clin Orthop. 2000;380:9–16. - PubMed
-
- Emerson R.H., Muncie M., Tarbox T.R., Higgins L.L. Comparison of a static with a mobile spacer in total knee infection. Clin Orthop. 2002;404:132–138. - PubMed
-
- Baleani M., Traina F., Toni A. The mechanical behaviour of a pre-formed hip spacer. HIP Int. 2003;13:159–162.
LinkOut - more resources
Full Text Sources
