

Pituitary stalk thickening in patients under 18 years of age - the most common causes and diagnostic procedures
- PMID: 35620922
- PMCID: PMC10214961
- DOI: 10.5114/pedm.2022.115202
Pituitary stalk thickening in patients under 18 years of age - the most common causes and diagnostic procedures
Abstract
Introduction: Pituitary stalk thickening (PST) is a rare abnormality in children, and it may be challenging due to its diverse clinical picture.
Aim of the study: The aim of the study is to summarize the data on the causes and diagnostic procedures of PST.
Material and methods: Papers were searched in the PubMed database identifying published randomized clinical trials, reviews, systematic reviews, meta-analyses, and case reports.
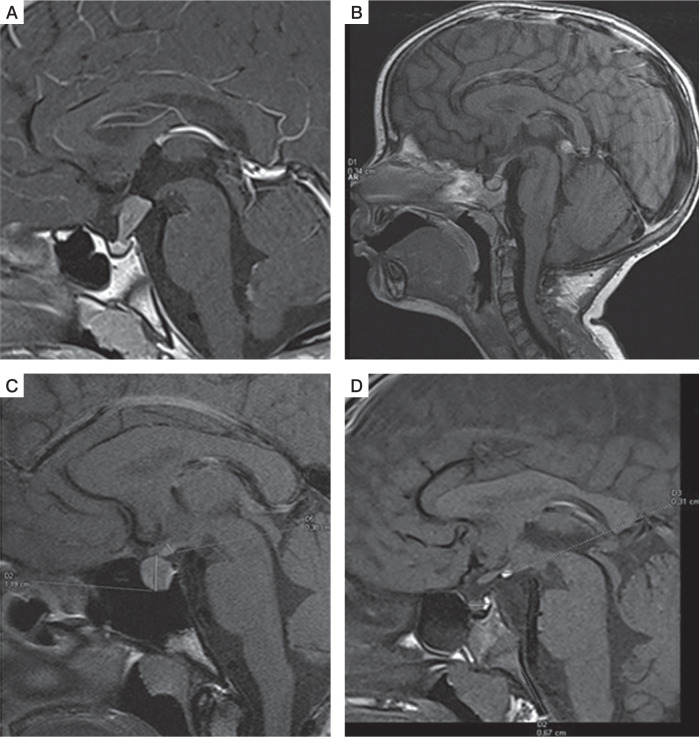
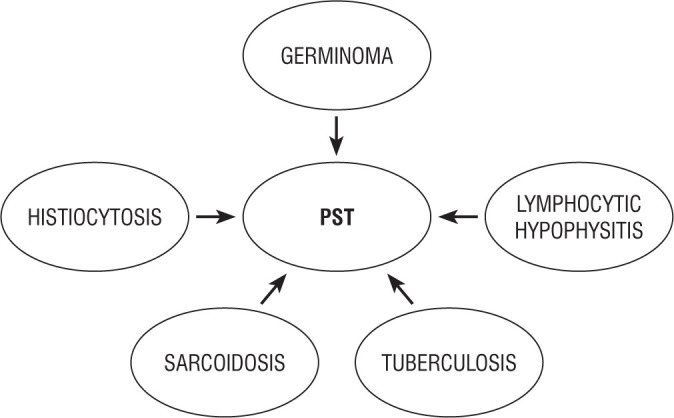
Results: The most common causes of a thickened pituitary stalk in children are germ cell tumours (GCTs), Langerhans cell histiocytosis (LCH), and lymphocytic infundibulo-neurohypophysitis (LINH). Neurosarcoidosis, pituitary tuberculosis, granulomatosis, or specific inflammations were only reported in the paediatric population as case studies. PST mainly affects teenagers and is often detected with brain magnetic resonance imaging (MRI) in patients with central diabetes insipidus (CDI). It is not possible to differentiate the causes of PST with the use of the MRI image alone. Although various biochemical and oncological markers and other imaging tests are used, the diagnosis of PST remains a significant diagnostic challenge for clinicians. The final diagnosis is made based on histopathological examination. The indications for a biopsy are not uniform. Most experts, including the authors of the 2021 British consensus, recommend biopsy in the case of PST with a stalk lesion diameter ≥ 6.5-7 mm.
Conclusions: The differential diagnosis of PST is a challenge. The diagnostic and treatment strategy should be individually adapted. Patients should be diagnosed in large clinical centres with experience in this field.
Wstęp: Pogrubienie szypuły przysadki (PST) jest rzadką nieprawidłowością u dzieci i trudnym problemem diagnostycznym ze względu na zróżnicowany obraz kliniczny.
Cel pracy: Podsumowanie danych dotyczących etiologii i diagnostyki PST.
Materiał i metody: Przegląd publikacji bazy PubMed obejmujący badania kliniczne z randomizacją, przeglądy systematyczne, metaanalizy, opisy przypadków.
Wyniki: Najczęstszymi przyczynami PST u dzieci są guzy zarodkowe (GCTs), histiocytoza z komórek Langerhansa (LCH) i limfocytarne zapalenie części nerwowej i szypuły przysadki (LINH). Z kolei neurosarkoidoza, gruźlica przysadki, ziarniniakowatość lub inne specyficzne stany zapalne przysadki w populacji pediatrycznej stanowią jedynie opisy przypadków. PST dotyczy głównie nastolatków i jest często wykrywane za pomocą rezonansu magnetycznego (MRI) mózgu u pacjentów z centralną moczówką prostą (CDI). Nie jest możliwe różnicowanie przyczyn PST na podstawie samego obrazu MRI. Pomimo dostępności markerów biochemicznych, onkologicznych oraz innych badań obrazowych rozpoznanie przyczyny PST pozostaje istotnym wyzwaniem diagnostycznym dla klinicystów. Ostateczną diagnozę stawia się na podstawie badania histopatologicznego. Wskazania do biopsji nie są jednolite. Większość ekspertów, w tym autorzy konsensusu brytyjskiego z 2021 r., zalecają biopsję w przypadku PST o średnicy zmiany w szypule ≥ 6,5–7 mm.
Wnioski: Diagnostyka różnicowa PST jest wyzwaniem. Strategia diagnostyczna i leczenie powinny być dostosowane indywidualnie do pacjenta i należy je przeprowadzać w dużych ośrodkach klinicznych mających doświadczenie w tej dziedzinie.
Keywords: diabetes insipidus; germinoma; histiocytosis; pituitary stalk thickening; children.
Conflict of interest statement
none declared.
Figures
Similar articles
-
Pituitary Stalk Thickening: Causes and Consequences. The Children's Memorial Health Institute Experience and Literature Review.Front Endocrinol (Lausanne). 2022 May 20;13:868558. doi: 10.3389/fendo.2022.868558. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35669693 Free PMC article. Review.
-
Central diabetes insipidus and pituitary stalk thickening in adults: distinction of neoplastic from non-neoplastic lesions.Eur J Endocrinol. 2020 Jul 1;181(3):95-105. doi: 10.1530/EJE-20-0058. Eur J Endocrinol. 2020. PMID: 32530258
-
Isolated Langerhans cell histiocytosis in the hypothalamic-pituitary region: a case report.BMC Endocr Disord. 2019 Dec 19;19(1):143. doi: 10.1186/s12902-019-0474-0. BMC Endocr Disord. 2019. PMID: 31856773 Free PMC article.
-
Thickened pituitary stalk on magnetic resonance imaging in children with central diabetes insipidus.Horm Res. 2000;53 Suppl 3:61-4. doi: 10.1159/000023536. Horm Res. 2000. PMID: 10971107 Clinical Trial.
-
[Central diabetes insipidus in adult patients--the first sign of Langerhans cell histiocytosis and Erdheim-Chester disease. Three case studies and literature review].Vnitr Lek. 2010 Feb;56(2):138-48. Vnitr Lek. 2010. PMID: 20329585 Review. Czech.
Cited by
-
Deficiency of arginine vasopressin in children - diagnostic and therapeutic approaches to improve patients' quality of life based on a 25-year, single-centre retrospective analysis.Pediatr Endocrinol Diabetes Metab. 2024;30(4):198-210. doi: 10.5114/pedm.2024.146684. Pediatr Endocrinol Diabetes Metab. 2024. PMID: 39963057 Free PMC article.
-
Incidence and Predictors for Oncologic Etiologies in Chinese Children with Pituitary Stalk Thickening.Cancers (Basel). 2023 Aug 2;15(15):3935. doi: 10.3390/cancers15153935. Cancers (Basel). 2023. PMID: 37568752 Free PMC article.
-
A 4-year-old Boy Positive for Anti-rabphilin-3A Antibody and Diagnosed With Lymphocytic Infundibuloneurohypophysitis.JCEM Case Rep. 2024 Dec 26;3(1):luae214. doi: 10.1210/jcemcr/luae214. eCollection 2025 Jan. JCEM Case Rep. 2024. PMID: 39726668 Free PMC article.
References
-
- Cai Y, Shou X, Zhang Z, et al. . Clinical features of patients with pituitary stalk thickening: a review of 159 cases from one medical center. Chin Neurosurg J 2017; 3: 2 10.1186/s41016-016-0070-3. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials