

Cerebral Circulation Time After Thrombectomy: A Potential Predictor of Outcome After Recanalization in Acute Stroke
- PMID: 35621204
- PMCID: PMC9238696
- DOI: 10.1161/JAHA.122.025853
Cerebral Circulation Time After Thrombectomy: A Potential Predictor of Outcome After Recanalization in Acute Stroke
Abstract
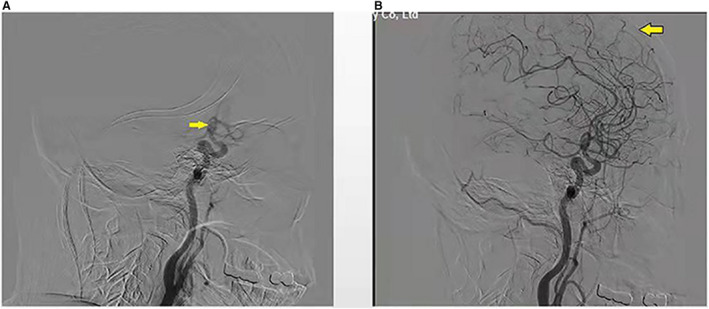
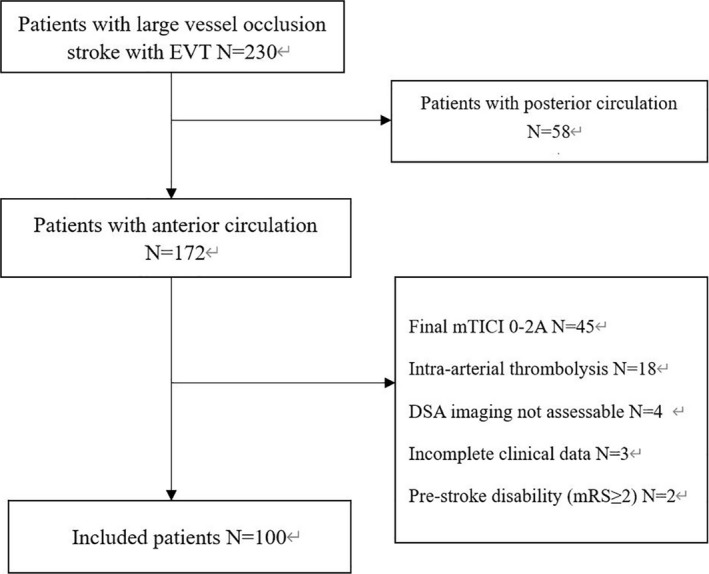
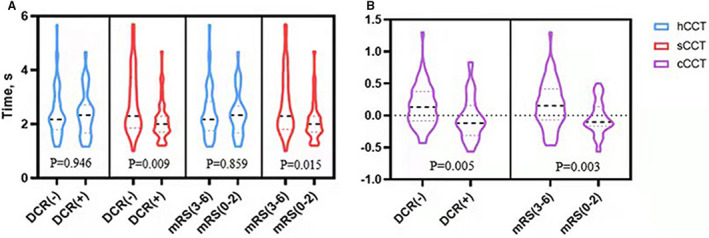
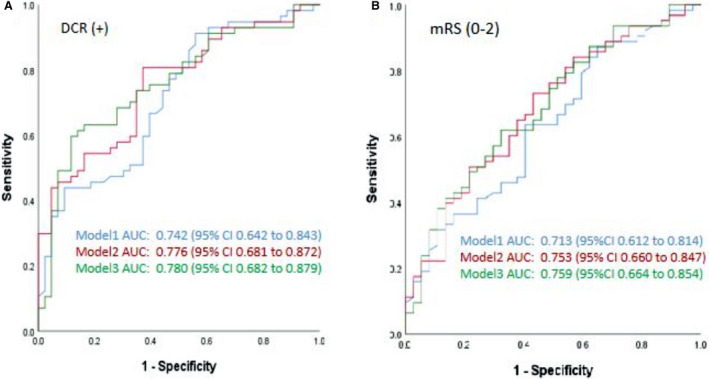
Background Despite successful recanalization, up to half of patients with acute ischemic stroke caused by large-vessel occlusion treated with endovascular treatment (EVT) do not recover to functional independence. We aim to evaluate the role of cerebral circulation time (CCT) as outcome predictor after EVT. Methods and Results We retrospectively enrolled consecutive patients with acute ischemic stroke-large-vessel occlusion undergoing EVT. Three categories of CCT based on digital subtraction angiography were studied: CCT of the stroke side, CCT of the healthy side), and change of CCT of the stroke side versus CCT of the healthy side. Dramatic clinical recovery was defined as a 24-hour National Institutes of Health Stroke Scale score ≤2 or ≥8 points drop. A modified Rankin Scale score ≤2 at 3 months was considered a favorable outcome. Logistic regression analysis was performed to evaluate the prediction of CCT on prognosis. One hundred patients were enrolled, of which 38 (38.0%) experienced a dramatic clinical recovery and 43 (43.0%) achieved a favorable outcome. Logistic regression analysis found that shorter change of CCT of the stroke side versus CCT of the healthy side and CCT of the stroke side were independent positive prognostic factors for dramatic clinical recovery (odds ratio [OR], 0.189; P=0.033; OR, 0.581; P=0.035) and favorable outcomes (OR, 0.142; P=0.020; OR, 0.581; P=0.046) after adjustment for potential confounders. A model including the change of CCT of the stroke side versus CCT of the healthy side also had significantly higher area under the curve values compared with the baseline model in patients with dramatic clinical recovery (0.780 versus 0.742) or favorable outcome (0.759 versus 0.713). Conclusions To our knowledge, this is the first report that CCT based on digital subtraction angiography data exhibits an independent predictive performance for clinical outcome in patients with acute ischemic stroke-large-vessel occlusion after EVT. Given that this readily available CCT can provide alternative perfusion information during EVT, a prospective, multicenter trial is warranted.
Keywords: cerebral circulation time; digital subtraction angiography; endovascular treatment; large‐vessel occlusion; outcome.
Figures
References
-
- Truelsen T, Hansen K, Andersen G, Sørensen L, Madsen C, Diaz A, Stavngaard T, Hundborg HH, Højgaard J, Hjort N, et al. Acute endovascular reperfusion treatment in patients with ischaemic stroke and large‐vessel occlusion (Denmark 2011–2017). Eur J Neurol. 2019;26:1044–1050. doi: 10.1111/ene.13931 - DOI - PubMed
-
- Bracard S, Ducrocq X, Mas JL, Soudant M, Oppenheim C, Moulin T, Guillemin F, THRACE investigators . Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurol. 2016;15:1138–1147. doi: 10.1016/S1474-4422(16)30177-6 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
