

Impact of S-Wave Amplitude in Right Precordial Leads on Improvement in Mitral Regurgitation following Cardiac Resynchronization Therapy
- PMID: 35621870
- PMCID: PMC9147072
- DOI: 10.3390/jcdd9050159
Impact of S-Wave Amplitude in Right Precordial Leads on Improvement in Mitral Regurgitation following Cardiac Resynchronization Therapy
Abstract
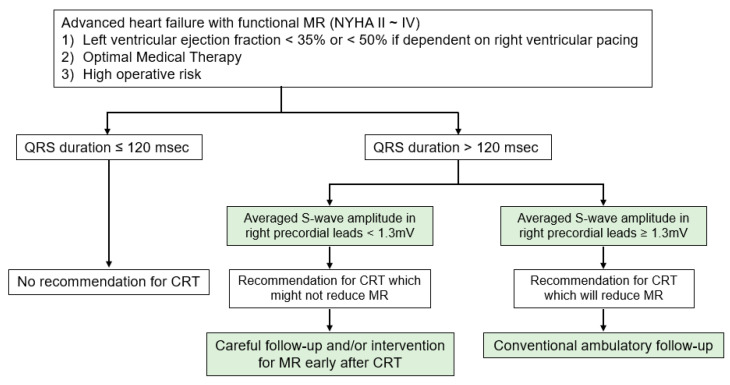
Background: The therapeutic strategy for mitral regurgitation (MR) in patients with advanced heart failure and wide QRS complex who are indicated for both intervention to MR and cardiac resynchronization therapy (CRT), remains unclear.
Objective: We aimed to determine electrocardiogram parameters that associate with MR reduction following CRT implantation.
Methods: Among the patients with advanced heart failure and functional MR who intended to receive CRT implantation, baseline QRS morphology, electrical axis, PR interval, QRS duration, and averaged S-wave in right precordial leads (V1 to V3) in surface electrocardiogram were measured. The impact of these parameters on MR reduction following CRT implantation, which was defined as a reduction in MR ≥1 grade six months later, was investigated.
Results: In 35 patients (median 71 years old, 18 men), 17 (49%) achieved an MR reduction following CRT implantation. Among baseline characteristics, only the higher S-wave amplitude in right precordial leads was an independent predictor of MR reduction (odds ratio 14.00, 95% confidence interval 1.65-119.00, p = 0.016) with a cutoff of 1.3 mV calculated through the area under the curve. The cutoff significantly stratified the cumulative incidences of heart failure re-admission and percutaneous mitral valve repair following CRT implantation (p = 0.032 and p = 0.011, respectively).
Conclusions: In patients with advanced heart failure and functional MR, the baseline higher amplitude of S-wave in the right precordial leads might be a good indicator of MR improvement following CRT.
Keywords: QRS amplitude; cardiac resynchronization therapy; heart failure.
Conflict of interest statement
The authors declare no conflict of interest associated with this manuscript.
Figures



Similar articles
-
A Simple Predictive Marker in Cardiac Resynchronization Therapy Recipients: Prominent S-Wave in Right Precordial Leads.Medicina (Kaunas). 2021 Aug 10;57(8):815. doi: 10.3390/medicina57080815. Medicina (Kaunas). 2021. PMID: 34441021 Free PMC article.
-
Assessing mitral regurgitation in the prediction of clinical outcome after cardiac resynchronization therapy.Heart Rhythm. 2015 Jun;12(6):1201-8. doi: 10.1016/j.hrthm.2015.02.022. Epub 2015 Feb 20. Heart Rhythm. 2015. PMID: 25708879
-
Native Electrocardiographic QRS Duration after Cardiac Resynchronization Therapy: The Impact on Clinical Outcomes and Prognosis.J Card Fail. 2016 Oct;22(10):772-80. doi: 10.1016/j.cardfail.2016.04.001. Epub 2016 Apr 4. J Card Fail. 2016. PMID: 27058406
-
Impact of cardiac resynchronization therapy on mitral valve apparatus geometry and clinical outcomes in patients with secondary mitral regurgitation.Echocardiography. 2017 Nov;34(11):1561-1567. doi: 10.1111/echo.13690. Epub 2017 Sep 12. Echocardiography. 2017. PMID: 28895197
-
QRS area as a predictor of cardiac resynchronization therapy response: A systematic review and meta-analysis.Pacing Clin Electrophysiol. 2022 Mar;45(3):393-400. doi: 10.1111/pace.14441. Epub 2022 Jan 29. Pacing Clin Electrophysiol. 2022. PMID: 35000207
References
-
- Van Bommel R.J., Marsan N.A., Delgado V., Borleffs C.J., van Rijnsoever E.P., Schalij M.J., Bax J.J. Cardiac resynchronization therapy as a therapeutic option in patients with moderate-severe functional mitral regurgitation and high operative risk. Circulation. 2011;124:912–919. doi: 10.1161/CIRCULATIONAHA.110.009803. - DOI - PubMed
-
- Yancy C.W., Jessup M., Bozkurt B., Butler J., Casey D.E., Jr., Drazner M.H., Fonarow G.C., Geraci S.A., Horwich T., Januzzi J.L., et al. American College of Cardiology Foundation. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 2013;62:e147–e239. doi: 10.1016/j.jacc.2013.05.019. - DOI - PubMed
-
- Ponikowski P., Voors A.A., Anker S.D., Bueno H., Cleland J.G.F., Coats A.J.S., Falk V., González-Juanatey J.R., Harjola V.P., Jankowska E.A., et al. ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016;37:2129–2200. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
