

Oncologist phenotypes and associations with response to a machine learning-based intervention to increase advance care planning: Secondary analysis of a randomized clinical trial
- PMID: 35622812
- PMCID: PMC9140236
- DOI: 10.1371/journal.pone.0267012
Oncologist phenotypes and associations with response to a machine learning-based intervention to increase advance care planning: Secondary analysis of a randomized clinical trial
Abstract
Background: While health systems have implemented multifaceted interventions to improve physician and patient communication in serious illnesses such as cancer, clinicians vary in their response to these initiatives. In this secondary analysis of a randomized trial, we identified phenotypes of oncology clinicians based on practice pattern and demographic data, then evaluated associations between such phenotypes and response to a machine learning (ML)-based intervention to prompt earlier advance care planning (ACP) for patients with cancer.
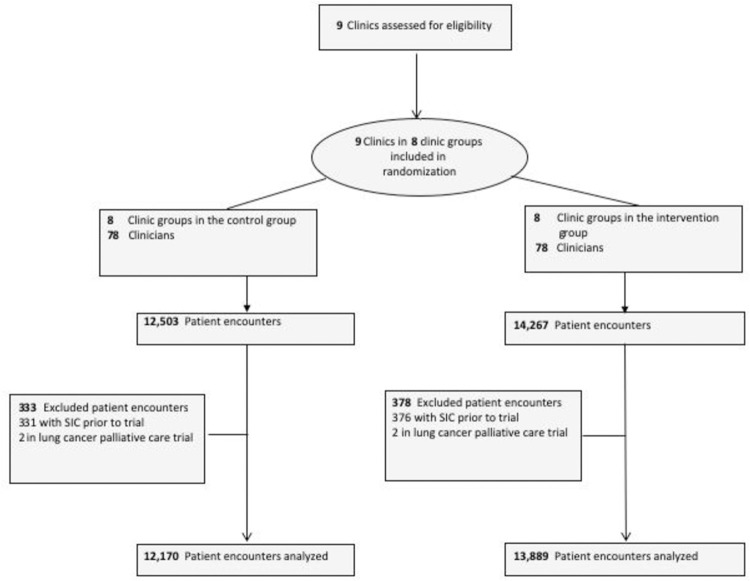
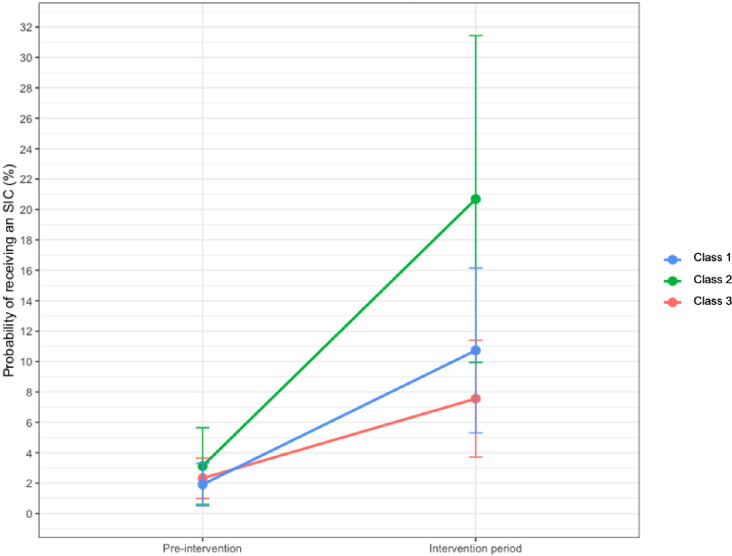
Methods and findings: Between June and November 2019, we conducted a pragmatic randomized controlled trial testing the impact of text message prompts to 78 oncology clinicians at 9 oncology practices to perform ACP conversations among patients with cancer at high risk of 180-day mortality, identified using a ML prognostic algorithm. All practices began in the pre-intervention group, which received weekly emails about ACP performance only; practices were sequentially randomized to receive the intervention at 4-week intervals in a stepped-wedge design. We used latent profile analysis (LPA) to identify oncologist phenotypes based on 11 baseline demographic and practice pattern variables identified using EHR and internal administrative sources. Difference-in-differences analyses assessed associations between oncologist phenotype and the outcome of change in ACP conversation rate, before and during the intervention period. Primary analyses were adjusted for patients' sex, age, race, insurance status, marital status, and Charlson comorbidity index. The sample consisted of 2695 patients with a mean age of 64.9 years, of whom 72% were White, 20% were Black, and 52% were male. 78 oncology clinicians (42 oncologists, 36 advanced practice providers) were included. Three oncologist phenotypes were identified: Class 1 (n = 9) composed primarily of high-volume generalist oncologists, Class 2 (n = 5) comprised primarily of low-volume specialist oncologists; and 3) Class 3 (n = 28), composed primarily of high-volume specialist oncologists. Compared with class 1 and class 3, class 2 had lower mean clinic days per week (1.6 vs 2.5 [class 3] vs 4.4 [class 1]) a higher percentage of new patients per week (35% vs 21% vs 18%), higher baseline ACP rates (3.9% vs 1.6% vs 0.8%), and lower baseline rates of chemotherapy within 14 days of death (1.4% vs 6.5% vs 7.1%). Overall, ACP rates were 3.6% in the pre-intervention wedges and 15.2% in intervention wedges (11.6 percentage-point difference). Compared to class 3, oncologists in class 1 (adjusted percentage-point difference-in-differences 3.6, 95% CI 1.0 to 6.1, p = 0.006) and class 2 (adjusted percentage-point difference-in-differences 12.3, 95% confidence interval [CI] 4.3 to 20.3, p = 0.003) had greater response to the intervention.
Conclusions: Patient volume and time availability may be associated with oncologists' response to interventions to increase ACP. Future interventions to prompt ACP should prioritize making time available for such conversations between oncologists and their patients.
Conflict of interest statement
This study was funded by a grant from the National Palliative Care Research Center. The authors have declared that no competing interests exist.
Figures
Similar articles
-
Effect of Integrating Machine Learning Mortality Estimates With Behavioral Nudges to Clinicians on Serious Illness Conversations Among Patients With Cancer: A Stepped-Wedge Cluster Randomized Clinical Trial.JAMA Oncol. 2020 Dec 1;6(12):e204759. doi: 10.1001/jamaoncol.2020.4759. Epub 2020 Dec 10. JAMA Oncol. 2020. PMID: 33057696 Free PMC article. Clinical Trial.
-
Hope and advance care planning in advanced cancer: Is there a relationship?Cancer. 2022 Mar 15;128(6):1339-1345. doi: 10.1002/cncr.34034. Epub 2021 Nov 17. Cancer. 2022. PMID: 34787930 Free PMC article. Clinical Trial.
-
Long-term Effect of Machine Learning-Triggered Behavioral Nudges on Serious Illness Conversations and End-of-Life Outcomes Among Patients With Cancer: A Randomized Clinical Trial.JAMA Oncol. 2023 Mar 1;9(3):414-418. doi: 10.1001/jamaoncol.2022.6303. JAMA Oncol. 2023. PMID: 36633868 Free PMC article. Clinical Trial.
-
Advance care planning for adults with heart failure.Cochrane Database Syst Rev. 2020 Feb 27;2(2):CD013022. doi: 10.1002/14651858.CD013022.pub2. Cochrane Database Syst Rev. 2020. PMID: 32104908 Free PMC article.
-
Does an Advance Care Planning Video Help Patients Having Surgery for Cancer Discuss Their Healthcare Preferences with Their Surgeons? [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2019 Apr. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2019 Apr. PMID: 37844164 Free Books & Documents. Review.
Cited by
-
Interventions aiming to improve advance care planning uptake in oncology: a scoping review of recent randomized controlled trials.Curr Opin Oncol. 2024 Jul 1;36(4):233-247. doi: 10.1097/CCO.0000000000001045. Epub 2024 May 9. Curr Opin Oncol. 2024. PMID: 38742390 Free PMC article.
-
Applying Machine Learning Techniques to Implementation Science.Online J Public Health Inform. 2024 Apr 22;16:e50201. doi: 10.2196/50201. Online J Public Health Inform. 2024. PMID: 38648094 Free PMC article.
-
Development of Machine Learning Algorithms Incorporating Electronic Health Record Data, Patient-Reported Outcomes, or Both to Predict Mortality for Outpatients With Cancer.JCO Clin Cancer Inform. 2022 Dec;6:e2200073. doi: 10.1200/CCI.22.00073. JCO Clin Cancer Inform. 2022. PMID: 36480775 Free PMC article.
-
The Use of Machine Learning for Analyzing Real-World Data in Disease Prediction and Management: Systematic Review.JMIR Med Inform. 2025 Jun 19;13:e68898. doi: 10.2196/68898. JMIR Med Inform. 2025. PMID: 40537090 Free PMC article.
-
Multidisciplinary clinician perceptions on utility of a machine learning tool (ALERT) to predict 6-month mortality and improve end-of-life outcomes for advanced cancer patients.Cancer Med. 2025 Mar;14(5):e70137. doi: 10.1002/cam4.70137. Cancer Med. 2025. PMID: 40029807 Free PMC article.
References
-
- Sanders JJ, Miller K, Desai M, Geerse OP, Paladino J, Kavanagh J, et al.. Measuring Goal-Concordant Care: Results and Reflections From Secondary Analysis of a Trial to Improve Serious Illness Communication. J Pain Symptom Manage. 2020. Nov 1;60(5):889–897.e2. doi: 10.1016/j.jpainsymman.2020.06.023 - DOI - PubMed
-
- Paladino J, Bernacki R, Neville BA, Kavanagh J, Miranda SP, Palmor M, et al.. Evaluating an Intervention to Improve Communication Between Oncology Clinicians and Patients With Life-Limiting Cancer: A Cluster Randomized Clinical Trial of the Serious Illness Care Program. JAMA Oncol. 2019. Jun 1;5(6):801. doi: 10.1001/jamaoncol.2019.0292 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
