

Effects of hospital facilities on patient outcomes after cancer surgery: an international, prospective, observational study
- PMID: 35623378
- PMCID: PMC9210173
- DOI: 10.1016/S2214-109X(22)00168-1
Effects of hospital facilities on patient outcomes after cancer surgery: an international, prospective, observational study
Abstract
Background: Early death after cancer surgery is higher in low-income and middle-income countries (LMICs) compared with in high-income countries, yet the impact of facility characteristics on early postoperative outcomes is unknown. The aim of this study was to examine the association between hospital infrastructure, resource availability, and processes on early outcomes after cancer surgery worldwide.
Methods: A multimethods analysis was performed as part of the GlobalSurg 3 study-a multicentre, international, prospective cohort study of patients who had surgery for breast, colorectal, or gastric cancer. The primary outcomes were 30-day mortality and 30-day major complication rates. Potentially beneficial hospital facilities were identified by variable selection to select those associated with 30-day mortality. Adjusted outcomes were determined using generalised estimating equations to account for patient characteristics and country-income group, with population stratification by hospital.
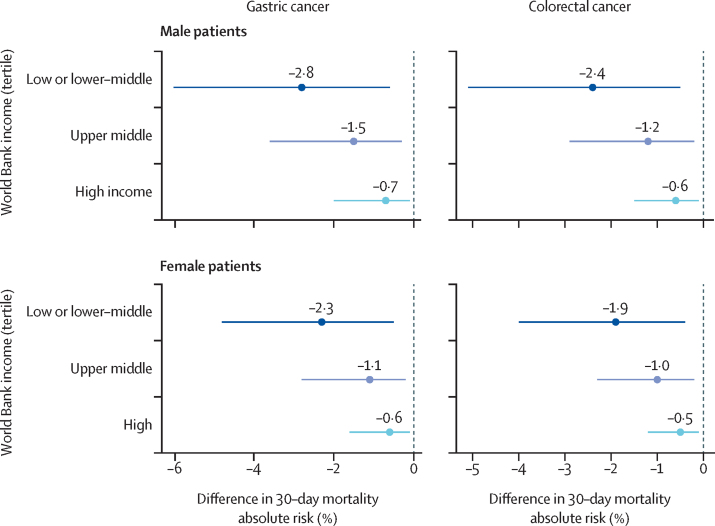
Findings: Between April 1, 2018, and April 23, 2019, facility-level data were collected for 9685 patients across 238 hospitals in 66 countries (91 hospitals in 20 high-income countries; 57 hospitals in 19 upper-middle-income countries; and 90 hospitals in 27 low-income to lower-middle-income countries). The availability of five hospital facilities was inversely associated with mortality: ultrasound, CT scanner, critical care unit, opioid analgesia, and oncologist. After adjustment for case-mix and country income group, hospitals with three or fewer of these facilities (62 hospitals, 1294 patients) had higher mortality compared with those with four or five (adjusted odds ratio [OR] 3·85 [95% CI 2·58-5·75]; p<0·0001), with excess mortality predominantly explained by a limited capacity to rescue following the development of major complications (63·0% vs 82·7%; OR 0·35 [0·23-0·53]; p<0·0001). Across LMICs, improvements in hospital facilities would prevent one to three deaths for every 100 patients undergoing surgery for cancer.
Interpretation: Hospitals with higher levels of infrastructure and resources have better outcomes after cancer surgery, independent of country income. Without urgent strengthening of hospital infrastructure and resources, the reductions in cancer-associated mortality associated with improved access will not be realised.
Funding: National Institute for Health and Care Research.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MIvBH reports personal fees from Mylan, Alesi Surgical, Johnson and Johnson, and Medtronic; grants and non-financial support from Stryker; and grants from Olympus, outside the submitted work; all fees were paid to their institution. PB reports grants and personal fees from the Medical Research Council; grants from National Institute for Health Research (NIHR) Health Technology Assessment and the Wellcome Trust; and personal fees from AG Biotest, outside the submitted work. TPK reports personal fees from Olympus Surgical, outside the submitted work. All other authors declare no competing interests.
Figures


Comment in
-
Do hospital facilities influence global cancer surgery outcomes?Lancet Glob Health. 2022 Jul;10(7):e936-e937. doi: 10.1016/S2214-109X(22)00214-5. Epub 2022 May 24. Lancet Glob Health. 2022. PMID: 35623377 No abstract available.
-
Surgery is really a team sport.Lancet Glob Health. 2022 Dec;10(12):e1713. doi: 10.1016/S2214-109X(22)00472-7. Lancet Glob Health. 2022. PMID: 36400082 No abstract available.
