

Morphological characteristics of the infrapatellar fat pad
- PMID: 35624138
- PMCID: PMC9142527
- DOI: 10.1038/s41598-022-12859-1
Morphological characteristics of the infrapatellar fat pad
Abstract
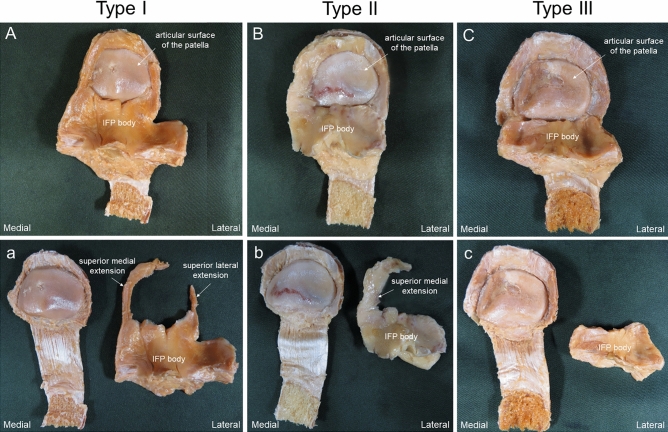
The relationship between the morphological characteristics of the infrapatellar fat pad (IFP) and joint deformity has yet to be fully elucidated. Therefore, the purpose of this study was to clarify the morphological characteristics of the IFP and to identify the relationships between morphological characteristics of the IFP and degenerative grade of the articular surface of the patella. This investigation examined 41 legs from 25 Japanese cadavers. The IFP length, width, and volume were measured. It was categorized into three types: Type I, IFP proximal located on medial and lateral sides of the patella; Type II, the IFP proximal only located medially; and Type III, absence of the IFP proximal. Articular surfaces were graded as macroscopically intact or mildly altered (Grade I), moderately (Grade II), or severely (Grade III). Grade III was significantly more frequent than Grades I or II in Type III. IFP volume was significantly larger in Type I than in Types II or III. A negative correlation was found between the degenerative grade of the articular surface of the patella and IFP volume. It was suggested that a relationship between the degenerative grade of the articular surface of the patella and the IFP volume.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
