

Hypoxia shapes the immune landscape in lung injury and promotes the persistence of inflammation
- PMID: 35624205
- PMCID: PMC9174051
- DOI: 10.1038/s41590-022-01216-z
Hypoxia shapes the immune landscape in lung injury and promotes the persistence of inflammation
Erratum in
-
Author Correction: Hypoxia shapes the immune landscape in lung injury and promotes the persistence of inflammation.Nat Immunol. 2022 Sep;23(9):1394. doi: 10.1038/s41590-022-01286-z. Nat Immunol. 2022. PMID: 35854097 Free PMC article. No abstract available.
Abstract
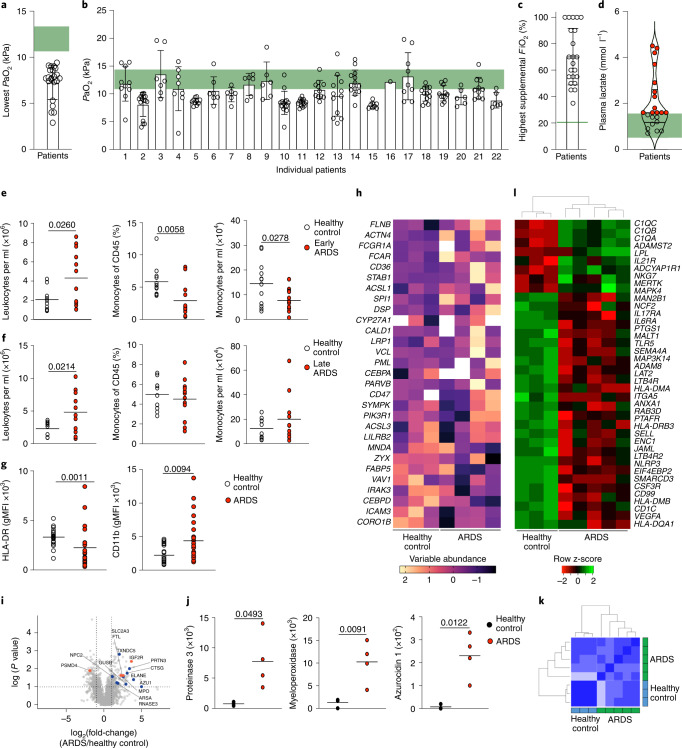
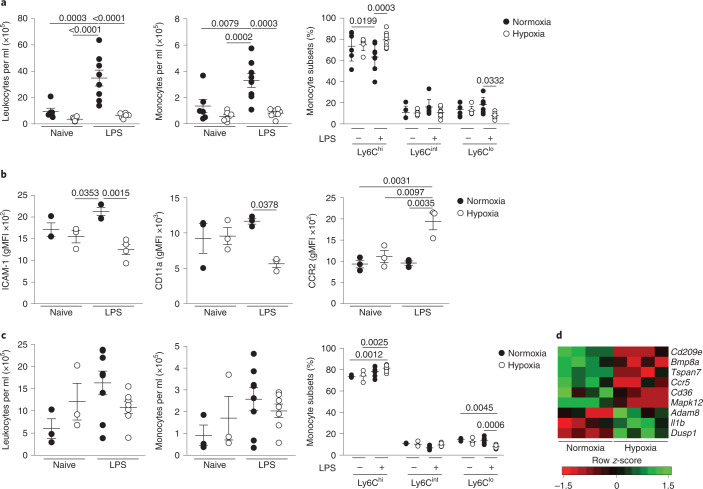
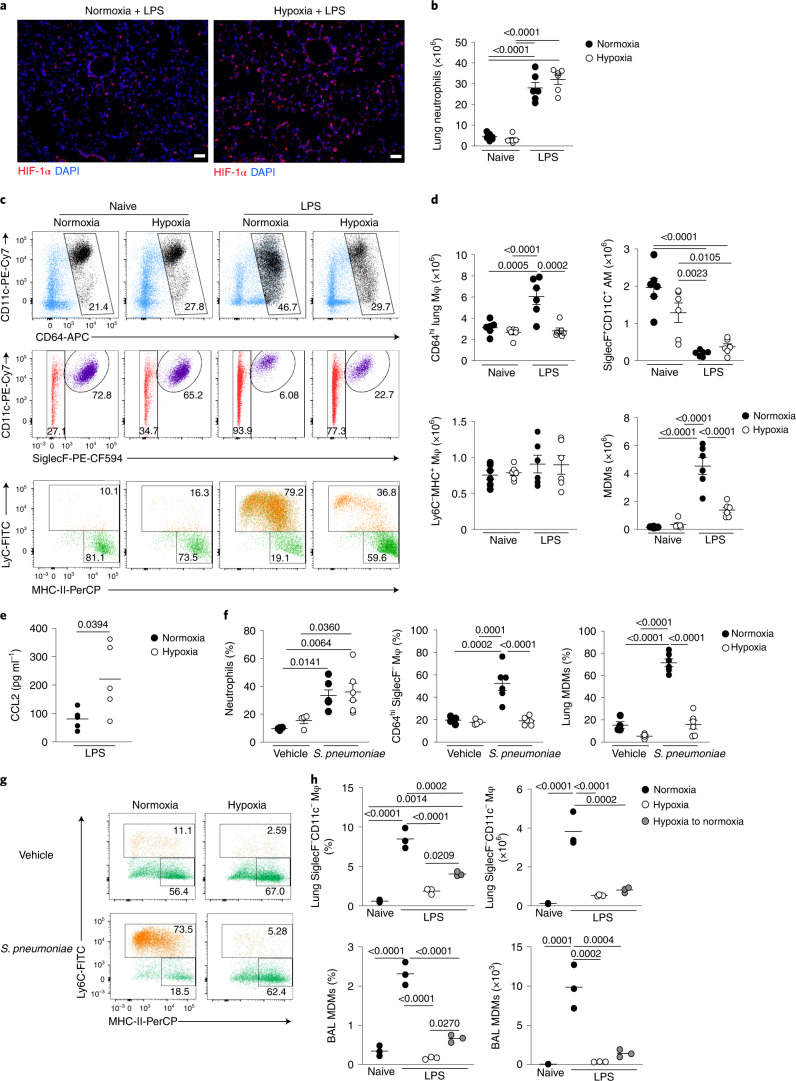
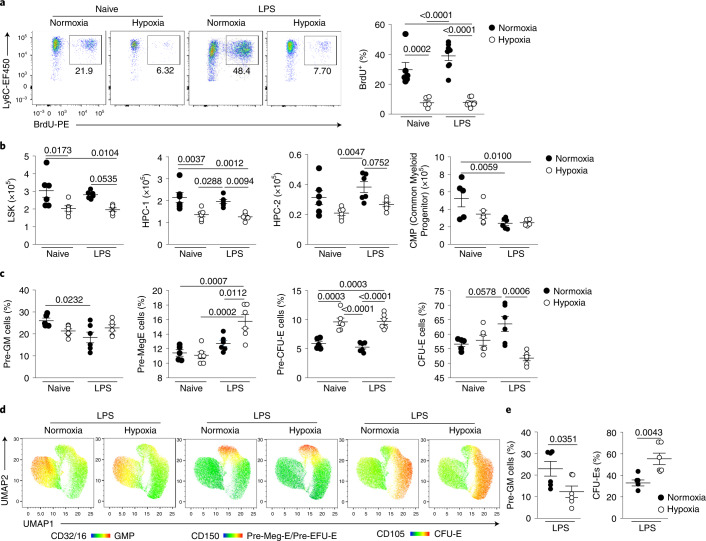
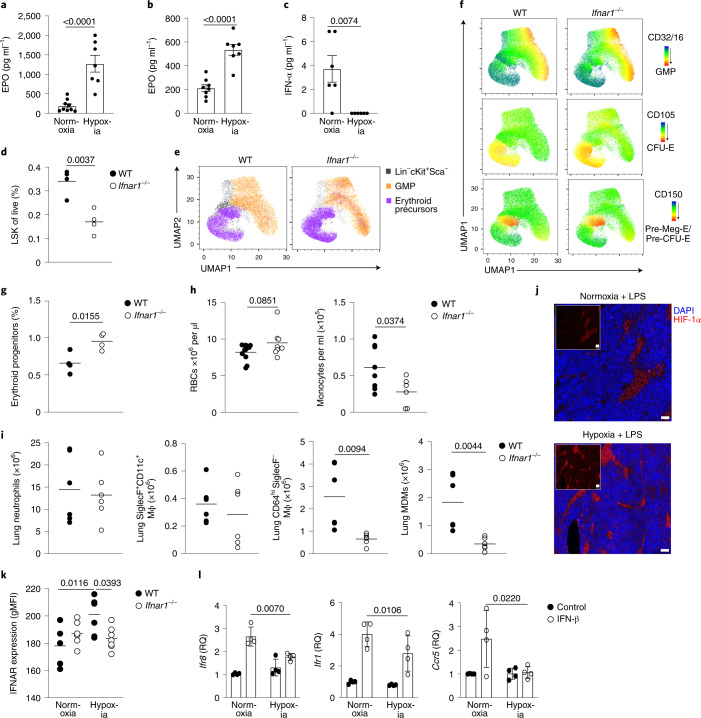
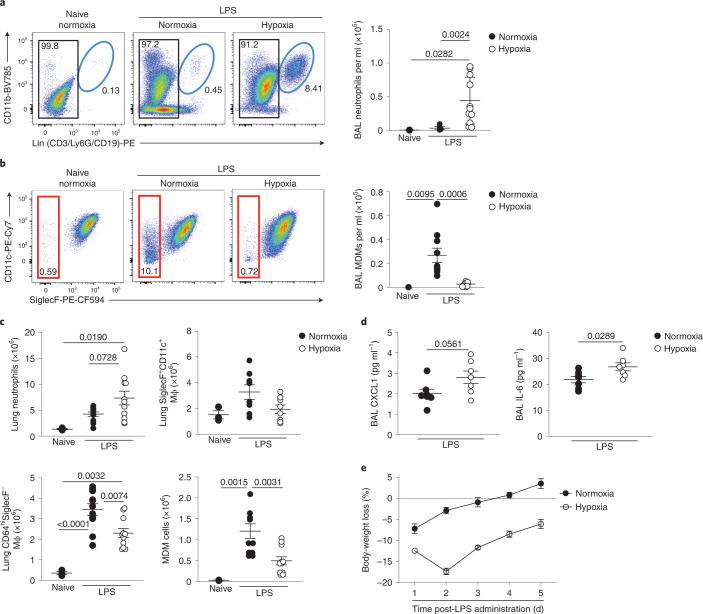
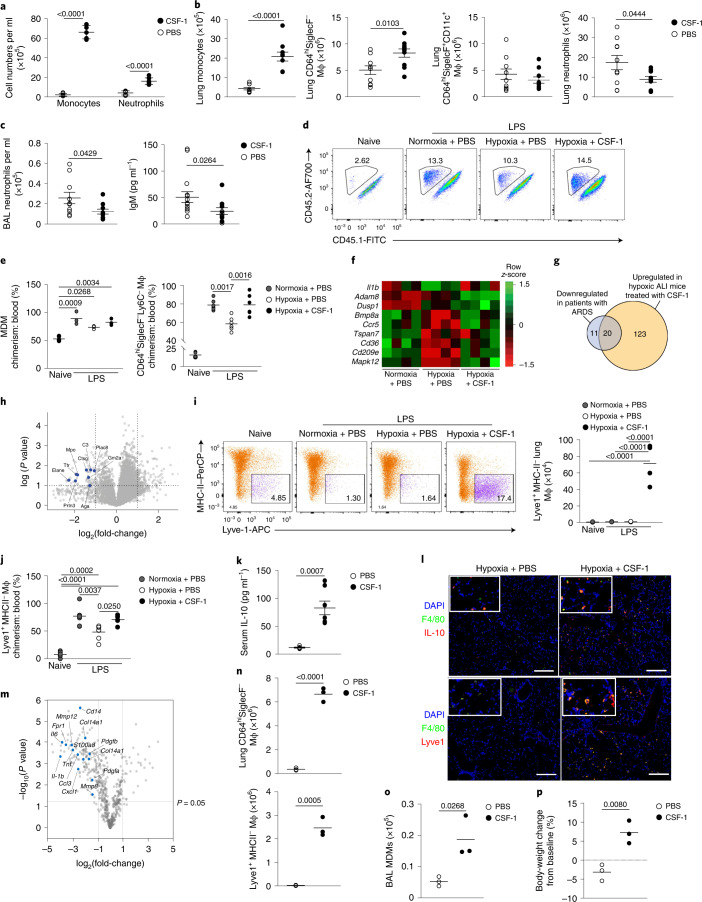
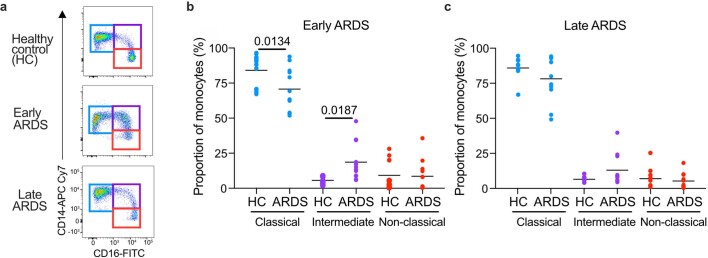
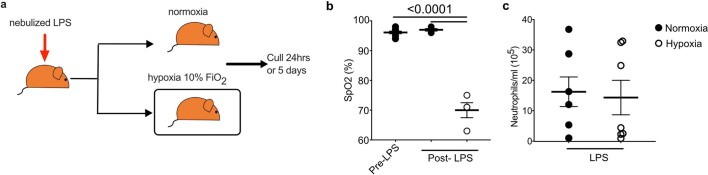
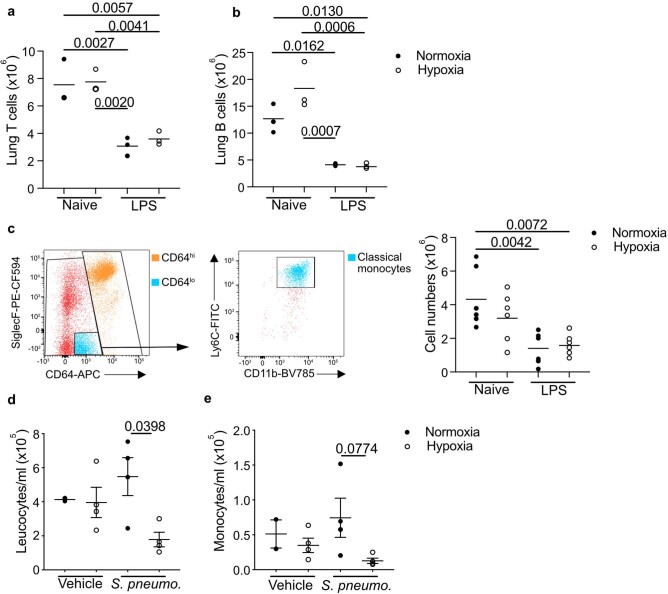
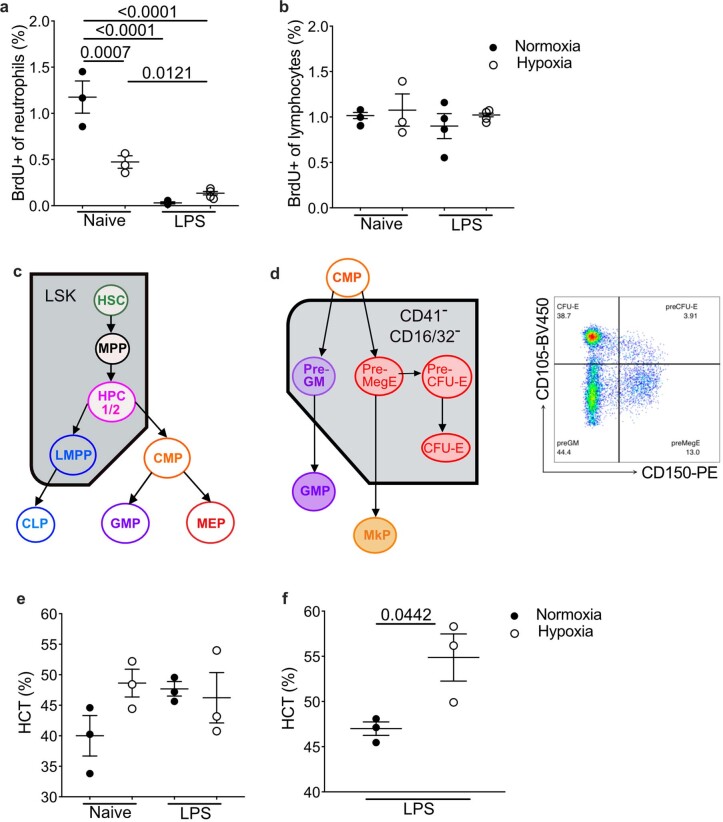
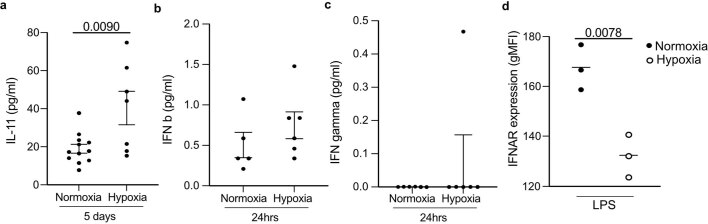
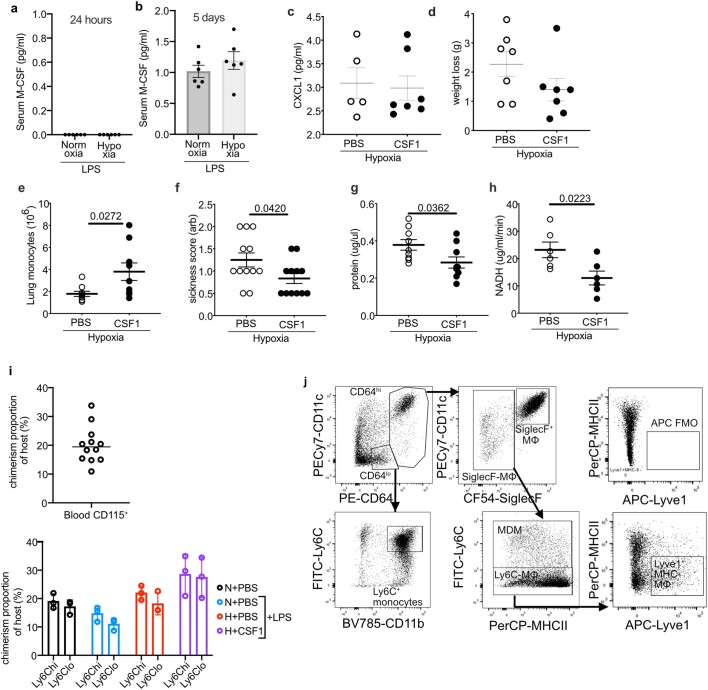
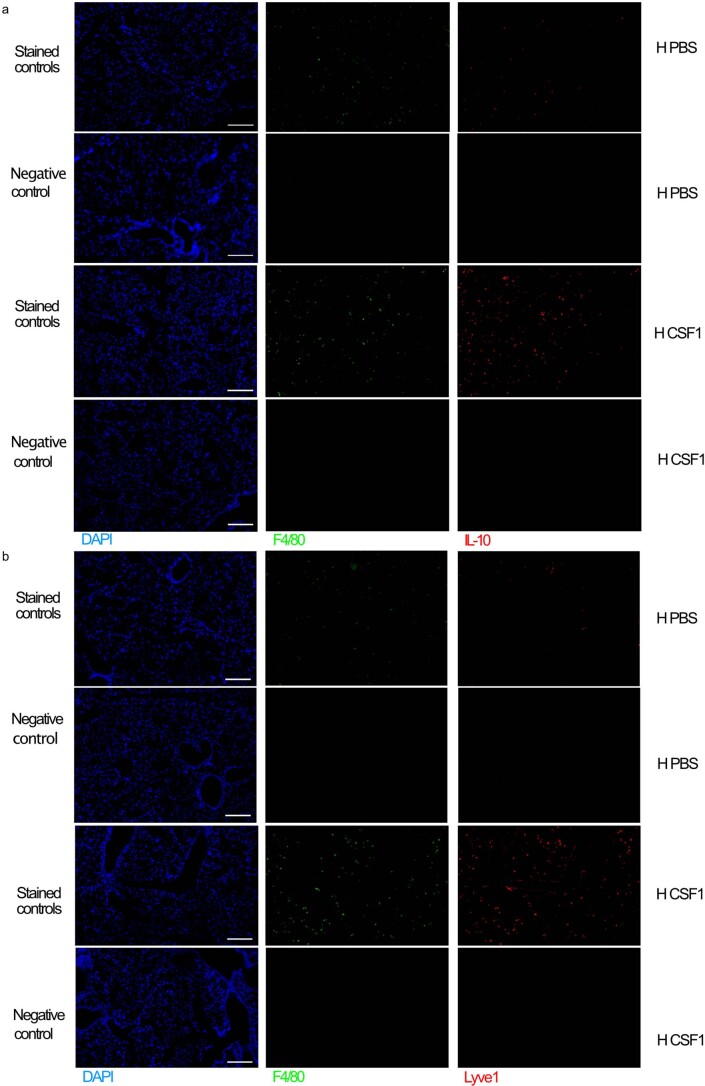
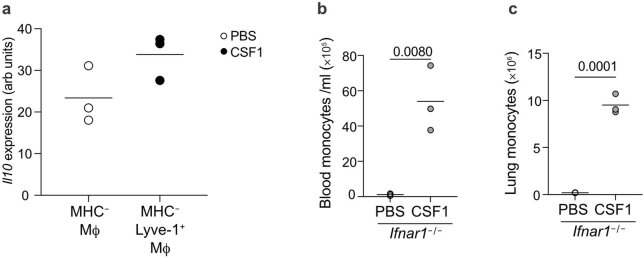
Hypoxemia is a defining feature of acute respiratory distress syndrome (ARDS), an often-fatal complication of pulmonary or systemic inflammation, yet the resulting tissue hypoxia, and its impact on immune responses, is often neglected. In the present study, we have shown that ARDS patients were hypoxemic and monocytopenic within the first 48 h of ventilation. Monocytopenia was also observed in mouse models of hypoxic acute lung injury, in which hypoxemia drove the suppression of type I interferon signaling in the bone marrow. This impaired monopoiesis resulted in reduced accumulation of monocyte-derived macrophages and enhanced neutrophil-mediated inflammation in the lung. Administration of colony-stimulating factor 1 in mice with hypoxic lung injury rescued the monocytopenia, altered the phenotype of circulating monocytes, increased monocyte-derived macrophages in the lung and limited injury. Thus, tissue hypoxia altered the dynamics of the immune response to the detriment of the host and interventions to address the aberrant response offer new therapeutic strategies for ARDS.
© 2022. The Author(s).
Conflict of interest statement
A.S.M., S.R.W., M.K.W., S.J.F. and S.J.J. have filed a patent for the use of CSF-1 as a therapy in ARDS with the University of Edinburgh (PCT/GB/2020/051184).
Figures
Comment in
-
A breath of fresh macrophages ameliorates inflammation in the hypoxic lung.Nat Immunol. 2022 Jun;23(6):820-822. doi: 10.1038/s41590-022-01214-1. Nat Immunol. 2022. PMID: 35624203 No abstract available.
References
-
- Fan E, et al. An official American Thoracic Society/European Society of intensive care medicine/society of critical care medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2017;195:1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- PIII052/WT_/Wellcome Trust/United Kingdom
- 206234/WT_/Wellcome Trust/United Kingdom
- DH_/Department of Health/United Kingdom
- 110086/WT_/Wellcome Trust/United Kingdom
- MR/T029668/1/MRC_/Medical Research Council/United Kingdom
- C29967/A26787/CRUK_/Cancer Research UK/United Kingdom
- 206211/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- MR/P019935/1/MRC_/Medical Research Council/United Kingdom
- 26787/CRUK_/Cancer Research UK/United Kingdom
- MR/P010008/1/MRC_/Medical Research Council/United Kingdom
- 209220/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- 098516/WT_/Wellcome Trust/United Kingdom
- MR/P010008/2/MRC_/Medical Research Council/United Kingdom
- 110086/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- MR/N02995X/1/MRC_/Medical Research Council/United Kingdom
- C29967A/14633/CRUK_/Cancer Research UK/United Kingdom
- 14633/CRUK_/Cancer Research UK/United Kingdom
- 209220/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
