

Robust hand tracking for surgical telestration
- PMID: 35624404
- PMCID: PMC9307534
- DOI: 10.1007/s11548-022-02637-9
Robust hand tracking for surgical telestration
Erratum in
-
Correction to: Robust hand tracking for surgical telestration.Int J Comput Assist Radiol Surg. 2022 Aug;17(8):1487. doi: 10.1007/s11548-022-02702-3. Int J Comput Assist Radiol Surg. 2022. PMID: 35802224 Free PMC article. No abstract available.
Abstract
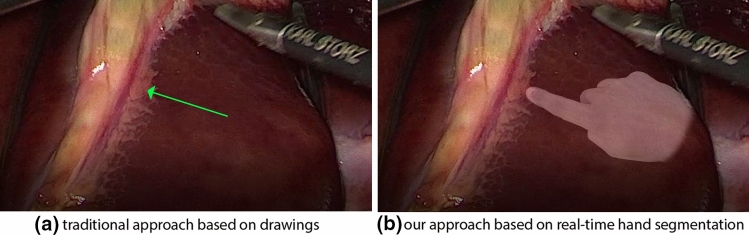
Purpose: As human failure has been shown to be one primary cause for post-operative death, surgical training is of the utmost socioeconomic importance. In this context, the concept of surgical telestration has been introduced to enable experienced surgeons to efficiently and effectively mentor trainees in an intuitive way. While previous approaches to telestration have concentrated on overlaying drawings on surgical videos, we explore the augmented reality (AR) visualization of surgical hands to imitate the direct interaction with the situs.
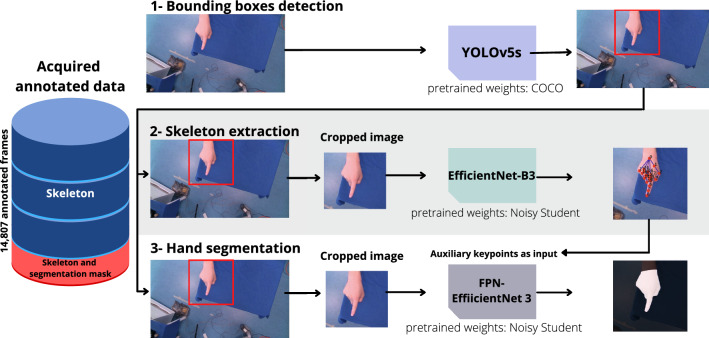
Methods: We present a real-time hand tracking pipeline specifically designed for the application of surgical telestration. It comprises three modules, dedicated to (1) the coarse localization of the expert's hand and the subsequent (2) segmentation of the hand for AR visualization in the field of view of the trainee and (3) regression of keypoints making up the hand's skeleton. The semantic representation is obtained to offer the ability for structured reporting of the motions performed as part of the teaching.
Results: According to a comprehensive validation based on a large data set comprising more than 14,000 annotated images with varying application-relevant conditions, our algorithm enables real-time hand tracking and is sufficiently accurate for the task of surgical telestration. In a retrospective validation study, a mean detection accuracy of 98%, a mean keypoint regression accuracy of 10.0 px and a mean Dice Similarity Coefficient of 0.95 were achieved. In a prospective validation study, it showed uncompromised performance when the sensor, operator or gesture varied.
Conclusion: Due to its high accuracy and fast inference time, our neural network-based approach to hand tracking is well suited for an AR approach to surgical telestration. Future work should be directed to evaluating the clinical value of the approach.
Keywords: Computer vision; Deep learning; Hand tracking; Surgical data science; Telestration.
© 2022. The Author(s).
Conflict of interest statement
LRM, JP, AY, PW, TJA, AS, KFK, BM, HK, FN, LMH do not declare conflicts of interest.
Figures





References
-
- Nepogodiev D, Martin J, Biccard B, Makupe A, Bhangu A, Ademuyiwa A, Adisa AO, Aguilera ML, Chakrabortee S, Fitzgerald JE, Ghosh D, Glasbey JC, Harrison EM, Ingabire JCA, Salem H, Lapitan MC, Lawani I, Lissauer D, Magill L, Moore R, Osei-Bordom DC, Pinkney TD, Qureshi AU, Ramos-De la Medina A, Rayne S, Sundar S, Tabiri S, Verjee A, Yepez R, Garden OJ, Lilford R, Brocklehurst P, Morton DG, Bhangu A (2019) Lobal burden of postoperative death. Lance. 10.1016/S0140-6736(18)33139-8
-
- Luck J, Hachach-Haram N, Greenfield M, Smith O, Billingsley M, Heyes R, Mosahebi A, Greenfield MJ. ugmented reality in undergraduate surgical training: the PROXIMIE pilot. Int J Surg. 2017 doi: 10.1016/j.ijsu.2017.08.029. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
