

Long-Term Follow-Up of Three Family Members with a Novel NNT Pathogenic Variant Causing Primary Adrenal Insufficiency
- PMID: 35627102
- PMCID: PMC9140979
- DOI: 10.3390/genes13050717
Long-Term Follow-Up of Three Family Members with a Novel NNT Pathogenic Variant Causing Primary Adrenal Insufficiency
Abstract
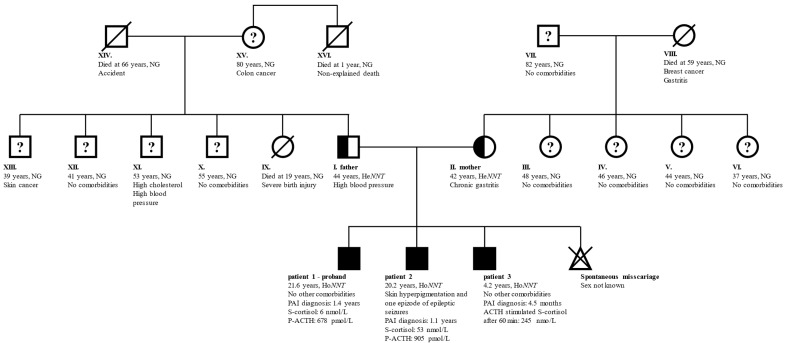
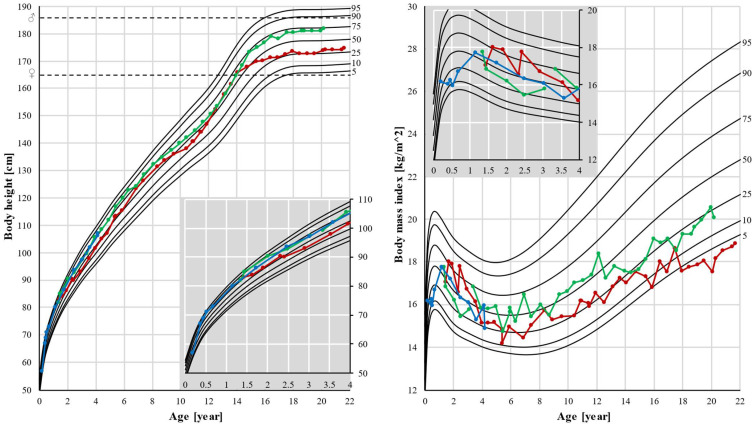
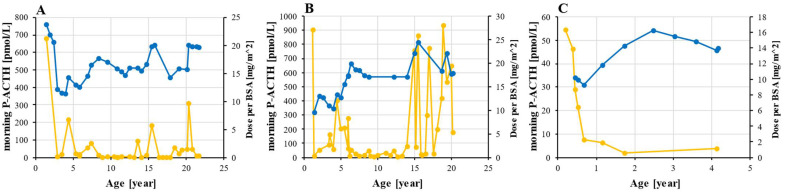
Nicotinamide nucleotide transhydrogenase (NNT) deficiency causes primary adrenal insufficiency (PAI) and possibly some extra-adrenal manifestations. A limited number of these patients were previously described. We present the clinical and genetic characteristics of three family members with a biallelic novel pathogenic variant in the NNT gene. The patients were followed until the ages of 21.6, 20.2, and 4.2 years. PAI was diagnosed in the eldest two brothers after an Addisonian crisis and the third was diagnosed at the age of 4.5 months in the asymptomatic stage due to the genetic screening of family members. Whole exome sequencing with a targeted interpretation of variants in genes related to PAI was performed in all the patients. The urinary steroid metabolome was determined by gas chromatography-mass spectrometry in the asymptomatic patient. The three patients, who were homozygous for c.1575dup in the NNT gene, developed isolated glucocorticoid deficiency. The urinary steroid metabolome showed normal excretion of cortisol metabolites. The adolescent patients had slow pubertal progression with low-normal testicular volume, while testicular endocrine function was normal. Bone mineral density was in the range for osteopenia in both grown-up siblings. Echocardiography revealed no structural or functional heart abnormalities. This article is among the first with a comprehensive and chronologically-detailed description of patients with NNT deficiency.
Keywords: NNT deficiency; bone density; hearth sonography; nicotinamide nucleotide transhydrogenase; nucleotide duplication; primary adrenal insufficiency; pubertal development; testicular volume.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Lack of NAD(P)+ transhydrogenase activity in patients with primary adrenal insufficiency due to NNT variants.Eur J Endocrinol. 2024 Feb 1;190(2):130-138. doi: 10.1093/ejendo/lvae011. Eur J Endocrinol. 2024. PMID: 38261461
-
A novel homozygous insertion and review of published mutations in the NNT gene causing familial glucocorticoid deficiency (FGD).Eur J Med Genet. 2015 Dec;58(12):642-9. doi: 10.1016/j.ejmg.2015.11.001. Epub 2015 Nov 6. Eur J Med Genet. 2015. PMID: 26548497 Review.
-
Combined adrenal failure and testicular adrenal rest tumor in a patient with nicotinamide nucleotide transhydrogenase deficiency.J Pediatr Endocrinol Metab. 2015 Sep;28(9-10):1187-90. doi: 10.1515/jpem-2015-0075. J Pediatr Endocrinol Metab. 2015. PMID: 25879317
-
NNT mutations: a cause of primary adrenal insufficiency, oxidative stress and extra-adrenal defects.Eur J Endocrinol. 2016 Jul;175(1):73-84. doi: 10.1530/EJE-16-0056. Epub 2016 Apr 29. Eur J Endocrinol. 2016. PMID: 27129361
-
Mitochondrial Nicotinamide Nucleotide Transhydrogenase: Role in Energy Metabolism, Redox Homeostasis, and Cancer.Antioxid Redox Signal. 2024 Nov;41(13-15):927-956. doi: 10.1089/ars.2024.0694. Antioxid Redox Signal. 2024. PMID: 39585234 Review.
Cited by
-
Addison's Disease: Diagnosis and Management Strategies.Int J Gen Med. 2023 Jun 2;16:2187-2210. doi: 10.2147/IJGM.S390793. eCollection 2023. Int J Gen Med. 2023. PMID: 37287503 Free PMC article. Review.
-
Metagenomic analysis of viral genes integrated in whole genome sequencing data of Thai patients with Brugada syndrome.Genomics Inform. 2022 Dec;20(4):e44. doi: 10.5808/gi.22047. Epub 2022 Dec 30. Genomics Inform. 2022. PMID: 36617651 Free PMC article.
-
Special Issue "Genetics and Epigenetics in Endocrine Disorders".Genes (Basel). 2023 Sep 5;14(9):1763. doi: 10.3390/genes14091763. Genes (Basel). 2023. PMID: 37761903 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
