

Uterine Fibroids and Pregnancy: A Review of the Challenges from a Romanian Tertiary Level Institution
- PMID: 35627994
- PMCID: PMC9141014
- DOI: 10.3390/healthcare10050855
Uterine Fibroids and Pregnancy: A Review of the Challenges from a Romanian Tertiary Level Institution
Abstract
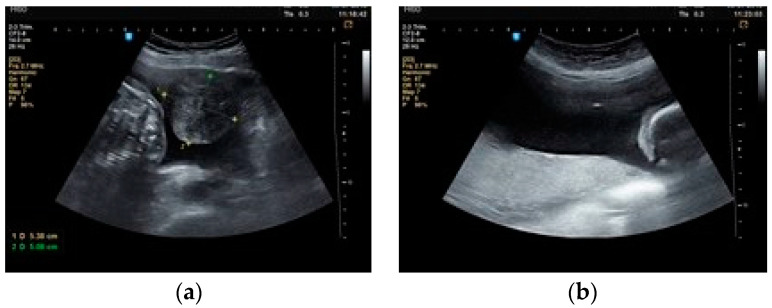
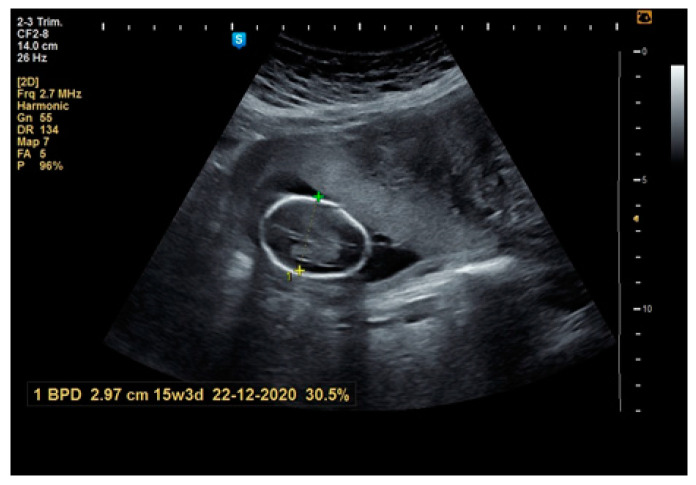
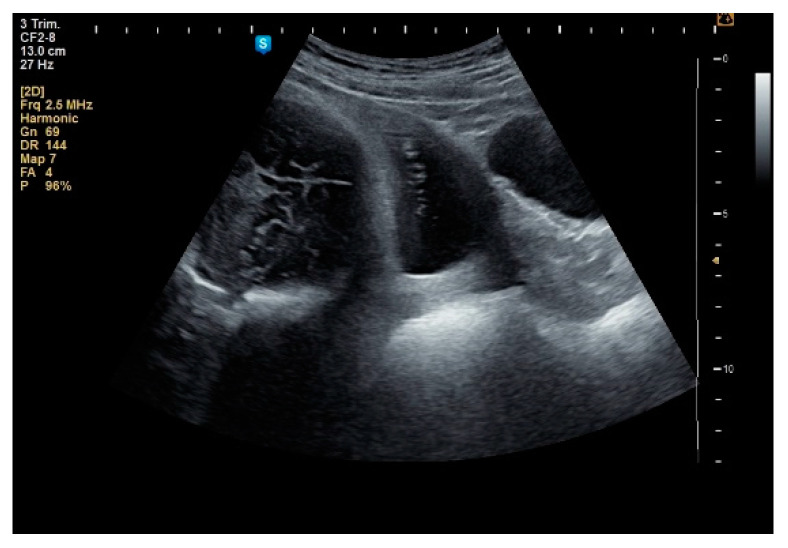
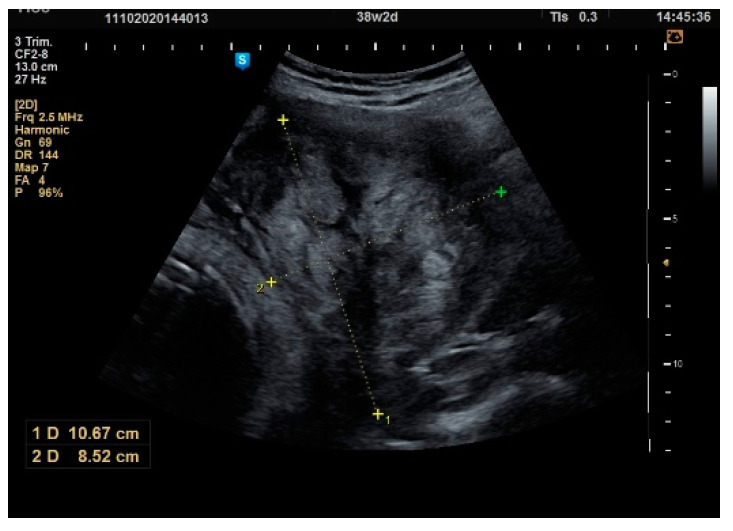
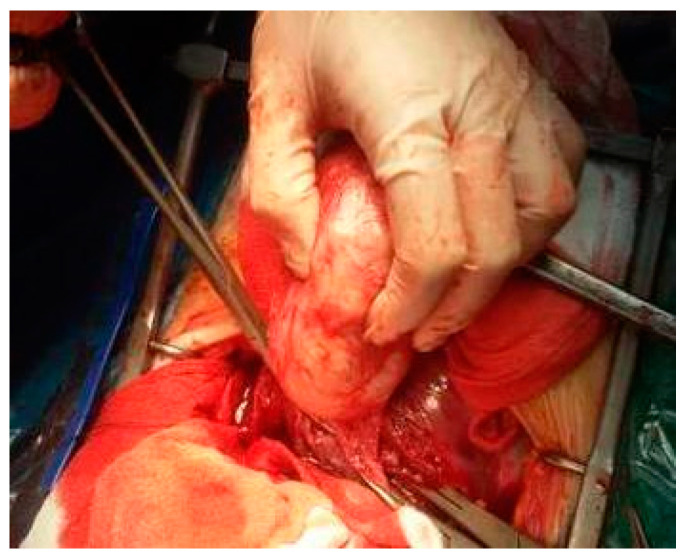
Background and objectives: Uterine fibroids are relatively common in reproductive-age women and are directly linked to pregnancy. There are many debates about performing a myomectomy at the same time as a caesarian section (CS) in such cases due to the risk of a hemorrhage. Our study aims to investigate fibroid features and their evolution in pregnancy, complications of a myomectomy during CS and maternal and fetal obstetric outcomes of pregnancies with fibroids.
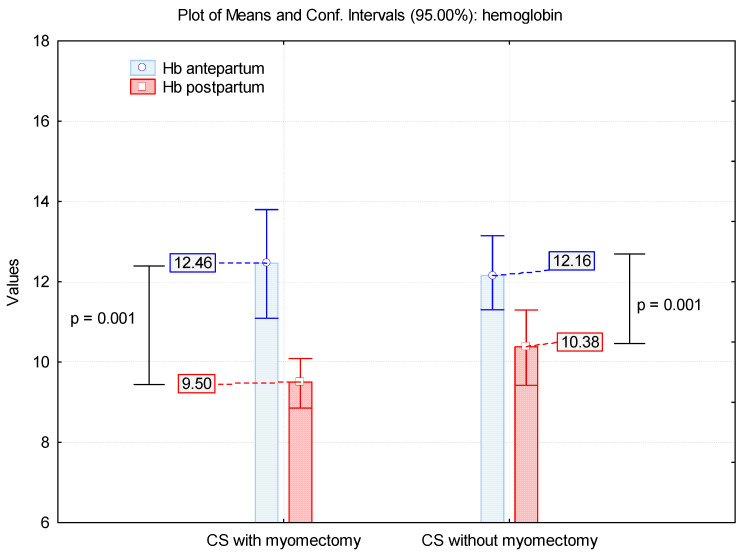
Materials and methods: We realize a prospective study that includes 57 patients with fibroids in pregnancy diagnosed in January 2017-June 2019. We analyze the number, the location and the growth of fibroids during pregnancy and the maternal and fetal outcome. We appreciate the bleeding in patients with a myomectomy and without a myomectomy during CS, using hemoglobin values before and after birth.
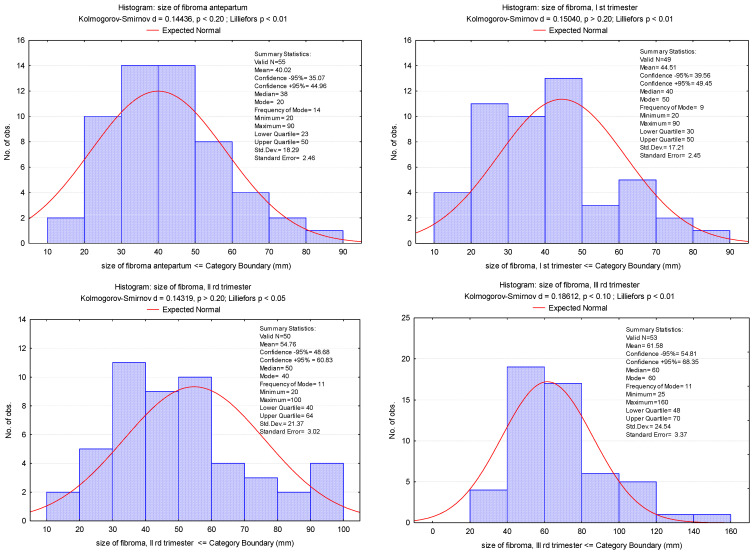
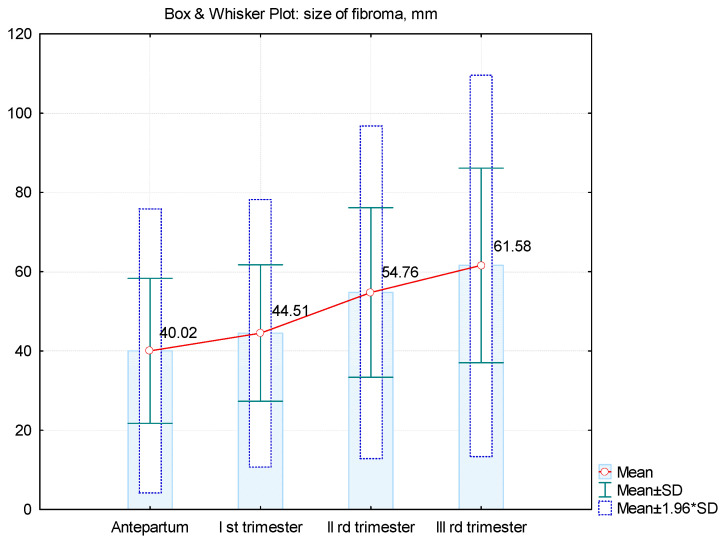
Results: Most of the patients present single fibroids that are 30-160 mm in size, located on the anterior uterine wall. Vaginal delivery is used in 7% of women, whereas 85.96% deliver by CS. In addition, 68% of fibroids are diagnosed in the first trimester. In most cases, the fibroid has maximum growth in the second trimester of pregnancy. The myomectomy rate for fibroids during CS is 24.48. Hemoglobin values showed no statistically significant difference between the two groups with and without myomectomy. The operating time is double for the group with a myomectomy associated with a CS. The results of the obstetric outcomes are abortion in 7% of all patients, whereas premature delivery and births at term are 9.43% and 90.57%, respectively.
Conclusions: The decision of performing a myomectomy during pregnancy can be a challenge and must be performed for selected cases. This procedure may have several benefits, such as avoiding another operation to remove fibroids.
Keywords: myomectomy; obstetric outcome; pregnancy; ultrasound; uterine fibroid.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources
