

Monoclonal Antibodies and Invasive Aspergillosis: Diagnostic and Therapeutic Perspectives
- PMID: 35628374
- PMCID: PMC9146623
- DOI: 10.3390/ijms23105563
Monoclonal Antibodies and Invasive Aspergillosis: Diagnostic and Therapeutic Perspectives
Abstract
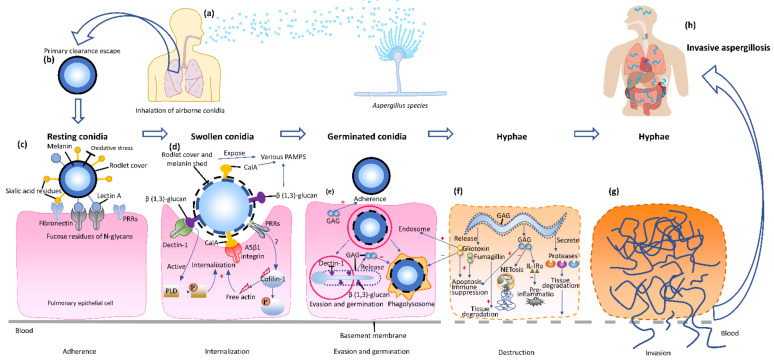
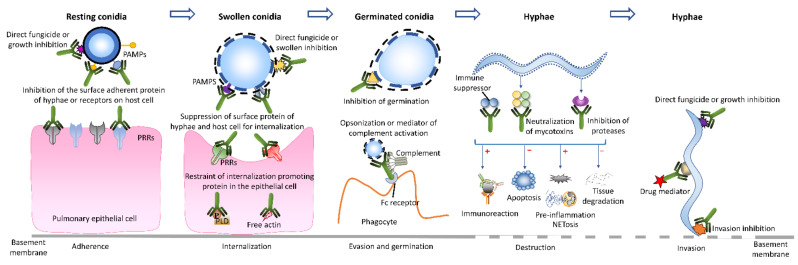
Invasive aspergillosis (IA) is a life-threatening fungal disease that causes high morbidity and mortality in immunosuppressed patients. Early and accurate diagnosis and treatment of IA remain challenging. Given the broad range of non-specific clinical symptoms and the shortcomings of current diagnostic techniques, most patients are either diagnosed as "possible" or "probable" cases but not "proven". Moreover, because of the lack of sensitive and specific tests, many high-risk patients receive an empirical therapy or a prolonged treatment of high-priced antifungal agents, leading to unnecessary adverse effects and a high risk of drug resistance. More precise diagnostic techniques alongside a targeted antifungal treatment are fundamental requirements for reducing the morbidity and mortality of IA. Monoclonal antibodies (mAbs) with high specificity in targeting the corresponding antigen(s) may have the potential to improve diagnostic tests and form the basis for novel IA treatments. This review summarizes the up-to-date application of mAb-based approaches in assisting IA diagnosis and therapy.
Keywords: Aspergillus infection; diagnosis; invasive aspergillosis; monoclonal antibody; therapy.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Jenks J.D., Gangneux J.P., Schwartz I.S., Alastruey-Izquierdo A., Lagrou K., Thompson Iii G.R., Lass-Florl C., Hoenigl M., European Confederation of Medical Mycology Council Investigators Diagnosis of breakthrough fungal infections in the clinical mycology laboratory: An ECMM consensus statement. J. Fungi. 2020;6:216. doi: 10.3390/jof6040216. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
