

Patterns of Recurrent Disease in Cervical Cancer
- PMID: 35629178
- PMCID: PMC9143345
- DOI: 10.3390/jpm12050755
Patterns of Recurrent Disease in Cervical Cancer
Abstract
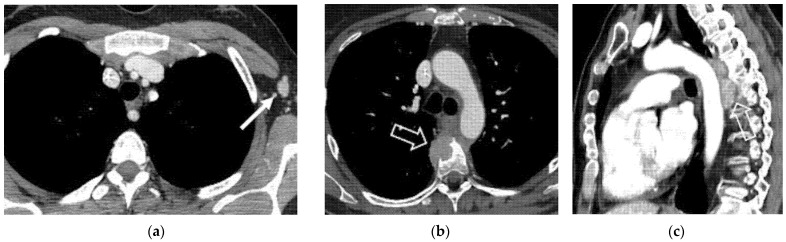
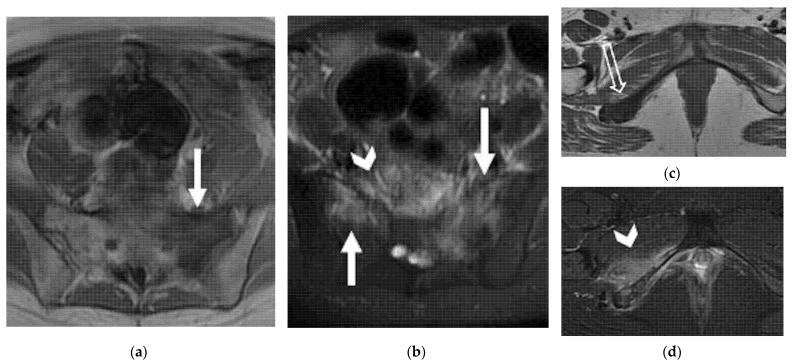
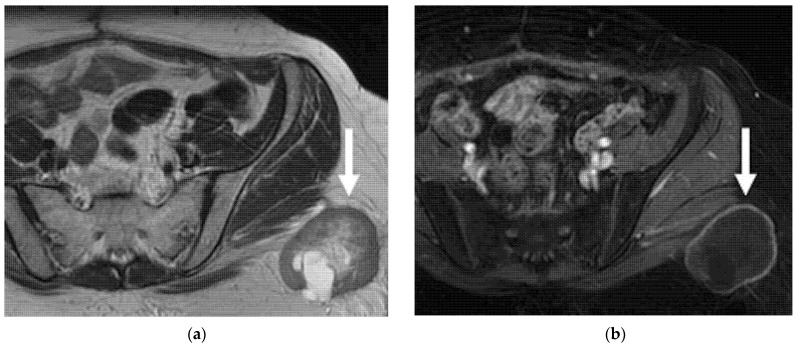
Uterine cervical cancer is one of the most common causes of cancer-related deaths among women worldwide. Patients with cervical cancer are at a high risk of pelvic recurrence or distant metastases within the first few years after primary treatment. However, no definitive agreement exists on the best post-treatment surveillance in these patients. Imaging may represent an accurate method of detecting relapse early, right when salvage treatment could be effective. In patients with recurrent cervical cancer, the correct interpretation of imaging may support the surgeon in the proper selection of patients prior to surgery to assess the feasibility of radical surgical procedure, or may help the clinician plan the most adaptive curative therapy. MRI can accurately define the extension of local recurrence and adjacent organ invasion; CT and 18F-FDG PET/CT may depict extra-pelvic distant metastases. This review illustrates different patterns of recurrent cervical cancer and how imaging, especially MRI, accurately contributes towards the diagnosis of local recurrence and the assessment of the extent of disease in patients with previous cervical cancer. Normal post-therapy pelvic appearance and possible pitfalls related to tissue changes for prior treatments will be also illustrated.
Keywords: CT; MRI; cervical cancer; personalized approach; recurrence.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Antunes D. Recurrent Cervical Cancer: How Can Radiology Be Helpfull. Omi. J. Radiol. 2013;2:138. doi: 10.4172/2167-7964.1000138. - DOI
-
- Bendifallah S., de Foucher T., Bricou A., Ouldamer L., Lavoue V., Varinot J., Canlorbe G., Carcopino X., Raimond E., Huguet F., et al. Cervical Cancer Recurrence: Proposal for a Classification Based on Anatomical Dissemination Pathways and Prognosis. Surg. Oncol. 2019;30:40–46. doi: 10.1016/j.suronc.2019.05.004. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
