

The Effect of Waning on Antibody Levels and Memory B Cell Recall following SARS-CoV-2 Infection or Vaccination
- PMID: 35632452
- PMCID: PMC9143792
- DOI: 10.3390/vaccines10050696
The Effect of Waning on Antibody Levels and Memory B Cell Recall following SARS-CoV-2 Infection or Vaccination
Abstract
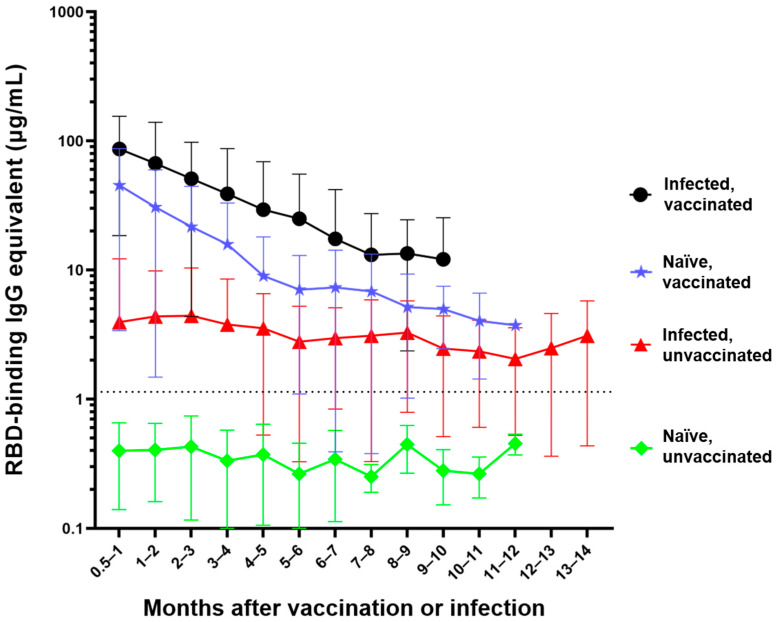
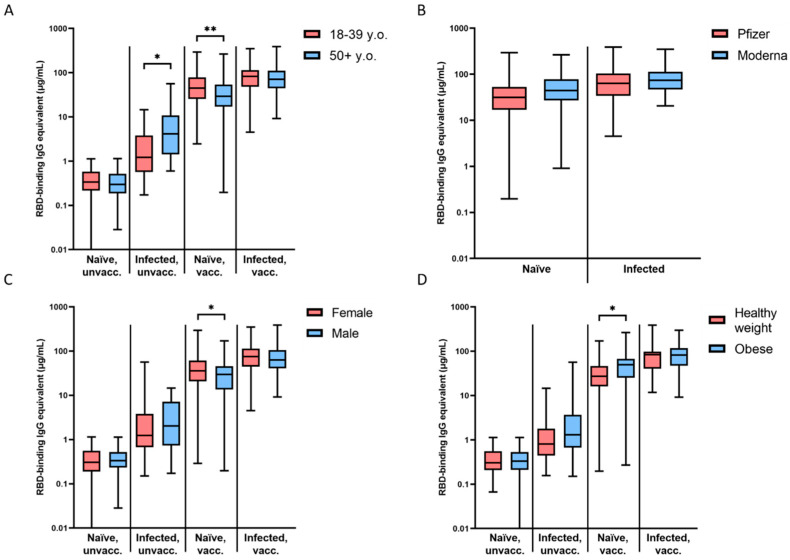
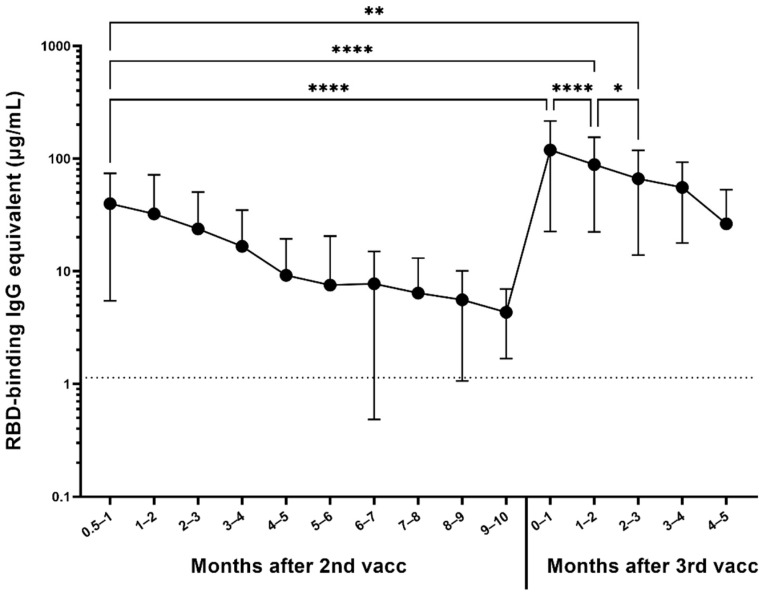
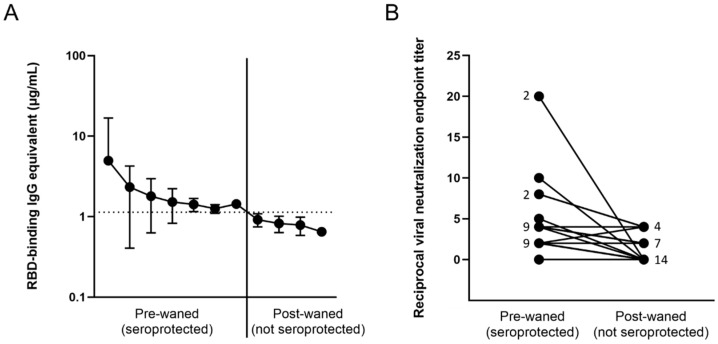
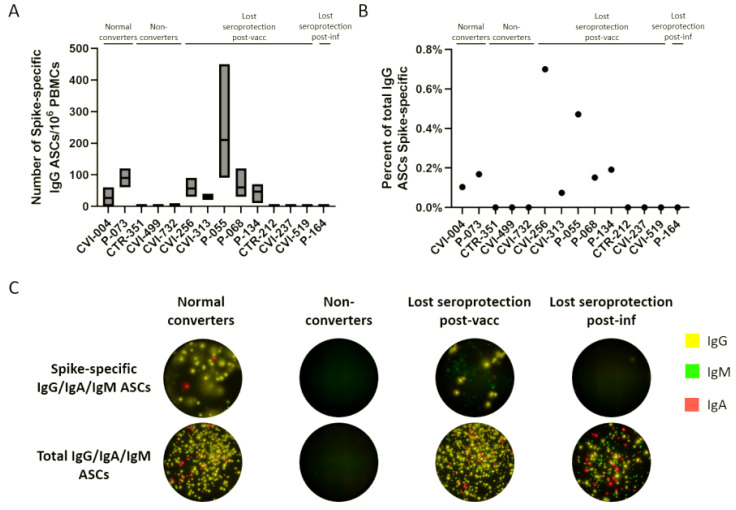
In order to longitudinally track SARS-CoV-2 antibody levels after vaccination or infection, we assessed anti-RBD antibody levels in over 1000 people and found no significant decrease in antibody levels during the first 14 months after infection in unvaccinated participants, however, a significant waning of antibody levels was observed following vaccination. Participants who were pre-immune to SARS-CoV-2 prior to vaccination seroconverted to higher antibody levels, which were maintained at higher levels than in previously infected, unvaccinated participants. Older participants exhibited lower level of antibodies after vaccination, but a higher level after infection than younger people. The rate of antibody waning was not affected by pre-immunity or age. Participants who received a third dose of an mRNA vaccine not only increased their antibody levels ~14-fold, but also had ~3 times more antibodies compared to when they received their primary vaccine series. PBMC-derived memory B cells from 13 participants who lost all circulating antibodies were differentiated into antibody secreting cells (ASCs). There was a significant recall of memory B cell ASCs in the absence of serum antibodies in 5-8 of the 10 vaccinated participants, but not in any of the 3 infected participants, suggesting a strong connection between antibody levels and the effectiveness of memory B cell recall.
Keywords: COVID-19; SARS-CoV-2; antibody decay; antibody secreting cells; infection; memory B cell recall; pre-immunity; vaccination; waning.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Update of
-
The effect of waning on antibody levels and memory B cell recall following SARS-CoV-2 infection or vaccination.bioRxiv [Preprint]. 2022 Mar 17:2022.03.16.484099. doi: 10.1101/2022.03.16.484099. bioRxiv. 2022. Update in: Vaccines (Basel). 2022 Apr 29;10(5):696. doi: 10.3390/vaccines10050696. PMID: 35313572 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
