

Analysis of early neonatal case fatality rate among newborns with congenital hydrocephalus, a 2000-2014 multi-country registry-based study
- PMID: 35633200
- PMCID: PMC9288486
- DOI: 10.1002/bdr2.2045
Analysis of early neonatal case fatality rate among newborns with congenital hydrocephalus, a 2000-2014 multi-country registry-based study
Abstract
Background: Congenital hydrocephalus (CH) comprises a heterogeneous group of birth anomalies with a wide-ranging prevalence across geographic regions and registry type. The aim of the present study was to analyze the early neonatal case fatality rate (CFR) and total birth prevalence of newborns diagnosed with CH.
Methods: Data were provided by 25 registries from four continents participating in the International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR) on births ascertained between 2000 and 2014. Two CH rates were calculated using a Poisson distribution: early neonatal CFR (death within 7 days) per 100 liveborn CH cases (CFR) and total birth prevalence rate (BPR) per 10,000 births (including live births and stillbirths) (BPR). Heterogeneity between registries was calculated using a meta-analysis approach with random effects. Temporal trends in CFR and BPR within registries were evaluated through Poisson regression modeling.
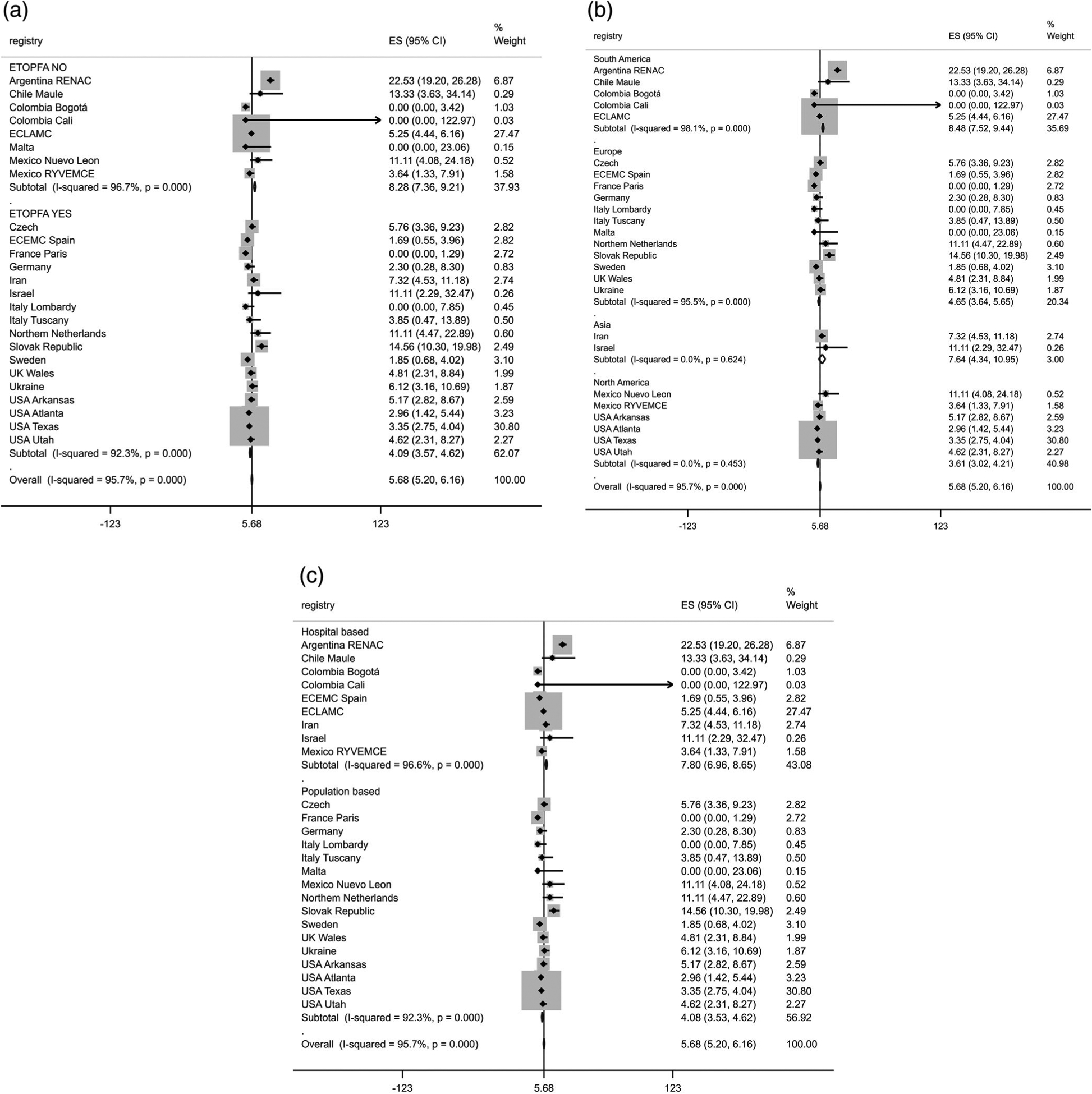
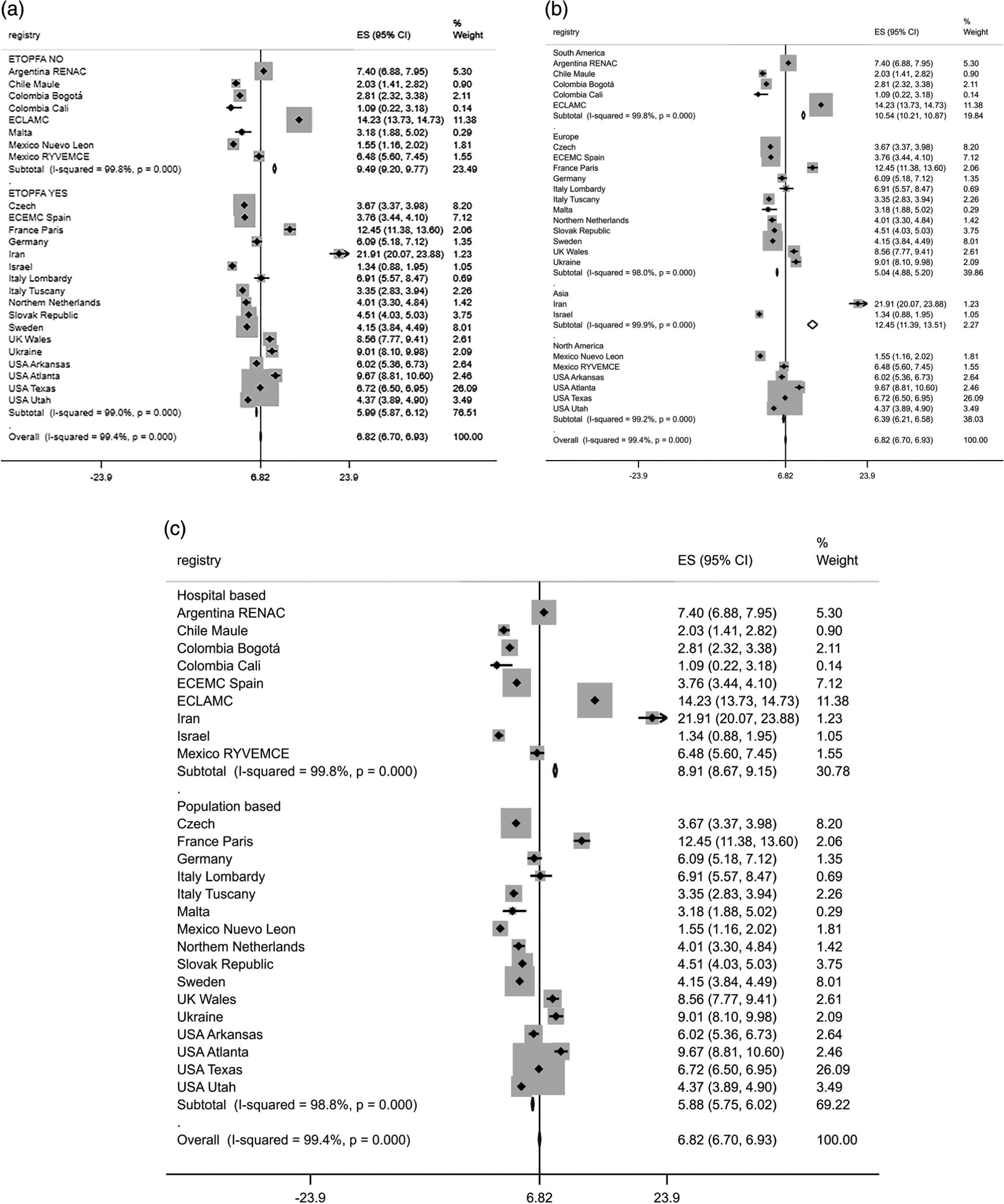
Results: A total of 13,112 CH cases among 19,293,280 total births were analyzed. The early neonatal CFR was 5.9 per 100 liveborn cases, 95% confidence interval (CI): 5.4-6.8. The CFR among syndromic cases was 2.7 times (95% CI: 2.2-3.3) higher than among non-syndromic cases (10.4% [95% CI: 9.3-11.7] and 4.4% [95% CI: 3.7-5.2], respectively). The total BPR was 6.8 per 10,000 births (95% CI: 6.7-6.9). Stratified by elective termination of pregnancy for fetal anomalies (ETOPFA), region and system, higher CFR were observed alongside higher BPR rates. The early neonatal CFR and total BPR did not show temporal variation, with the exception of a CFR decrease in one registry.
Conclusions: Findings of early neonatal CFR and total BPR were highly heterogeneous among registries participating in ICBDSR. Most registries with higher CFR also had higher BPR. Differences were attributable to type of registry (hospital-based vs. population-based), ETOPFA (allowed yes or no) and geographical regions. These findings contribute to the understanding of regional differences of CH occurrence and early neonatal deaths.
Keywords: ETOPFA; birth defects; case fatality rate; congenital hydrocephalus; early neonatal deaths; population surveillance; prevalence; trends.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
CONFLICT OF INTERESTS
The authors declare that they have no competing interests in publishing this manuscript. The authors received no funding for this analysis.
Figures
References
-
- Alijahan R, Mirzarahimi M, Ahmadi Hadi P, & Hazrati S (2013). Prevalence of congenital abnormalities and its related risk factors in Ardabil, Iran, 2011. The Iranian Journal of Obstetrics, Gynecology and Infertility, 16(54), 16–25. 10.22038/ijogi.2013.1086 - DOI
-
- Bakker MK, Kancherla V, Canfield MA, Bermejo-Sanchez E, Cragan JD, Dastgiri S, … Mastroiacovo P (2019). Analysis of mortality among neonates and children with spina bifida: An international registry-based study, 2001–2012. Paediatric and Perinatal Epidemiology, 33(6), 436–448. 10.1111/ppe.12589 - DOI - PMC - PubMed
-
- Best KE, Rankin J, Dolk H, Loane M, Haeusler M, Nelen V, … Khoshnood B (2020). Multilevel analyses of related public health indicators: The European Surveillance of Congenital Anomalies (EUROCAT) Public Health Indicators. Paediatric and Perinatal Epidemiology, 34(2), 122–129. 10.1111/ppe.12655 - DOI - PMC - PubMed
-
- Bradburn M, Deeks J, & Altman DG (1998). metan—An alternative meta-analysis command. Stata Techicall Bulletin, 44, 4–15.
-
- Daliri S, Safarpour H, Bazyar J, Sayehmiri K, Karimi A, & Anvary R (2019). The relationship between some neonatal and maternal factors during pregnancy with the prevalence of congenital malformations in Iran: A systematic review and meta-analysis. The Journal of Maternal-Fetal & Neonatal Medicine: The Official Journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, 32(21), 3666–3674. 10.1080/14767058.2018.1465917 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
