

Characteristics, phenotypes, mechanisms and management of severe asthma
- PMID: 35633594
- PMCID: PMC9337252
- DOI: 10.1097/CM9.0000000000001990
Characteristics, phenotypes, mechanisms and management of severe asthma
Abstract
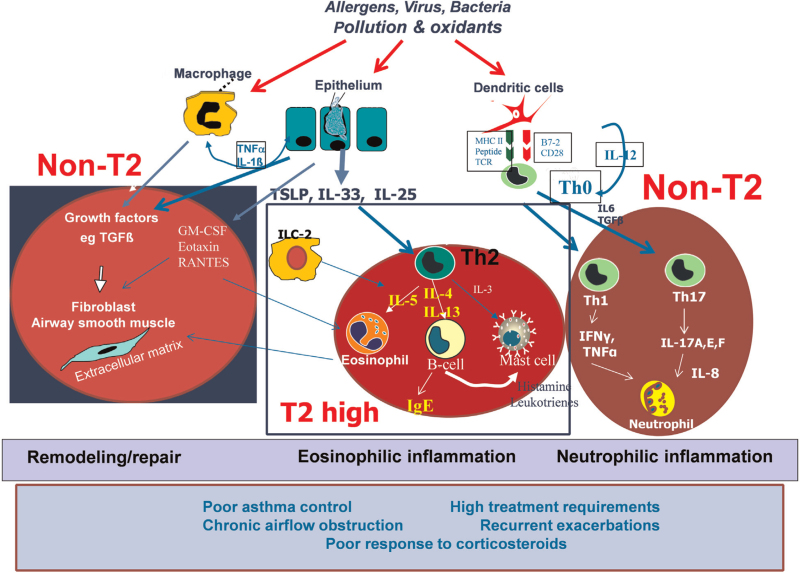
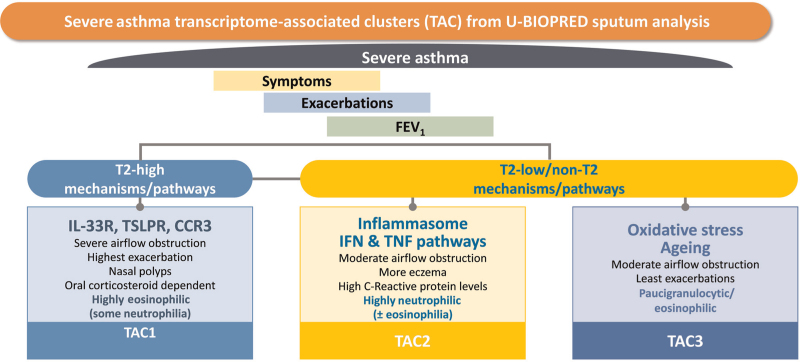
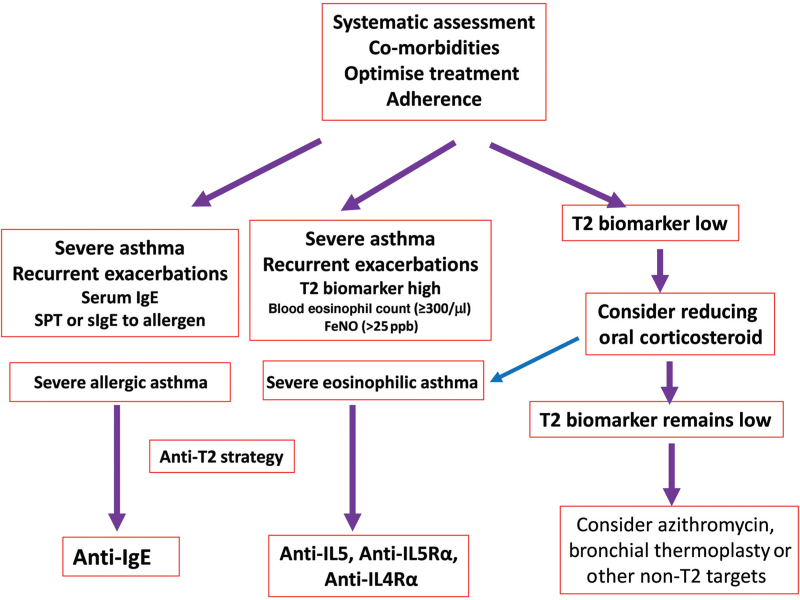
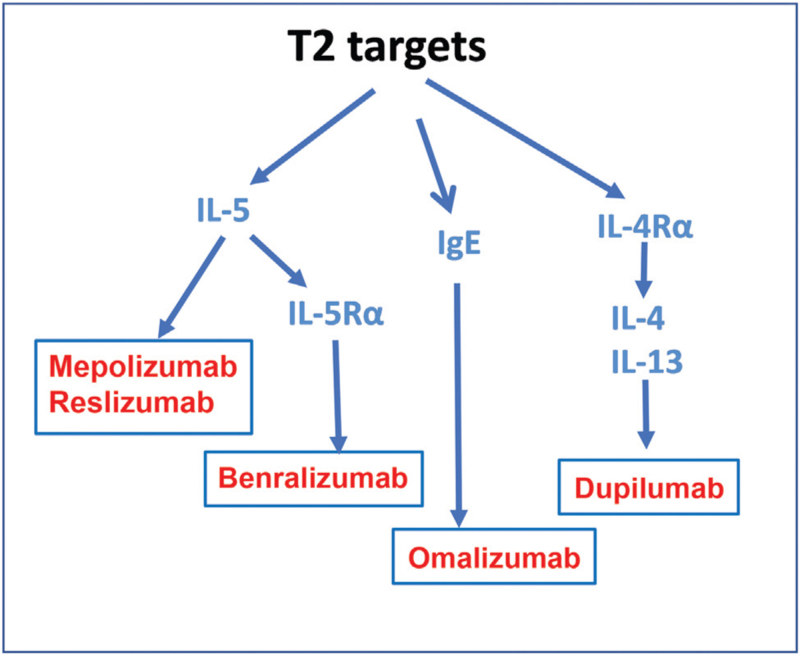
Severe asthma is "asthma which requires treatment with high dose inhaled corticosteroids (ICS) plus a second controller (and/or systemic corticosteroids) to prevent it from becoming 'uncontrolled' or which remains 'uncontrolled' despite this therapy." The state of control was defined by symptoms, exacerbations and the degree of airflow obstruction. Therefore, for the diagnosis of severe asthma, it is important to have evidence for a diagnosis of asthma with an assessment of its severity, followed by a review of comorbidities, risk factors, triggers and an assessment of whether treatment is commensurate with severity, whether the prescribed treatments have been adhered to and whether inhaled therapy has been properly administered. Phenotyping of severe asthma has been introduced with the definition of a severe eosinophilic asthma phenotype characterized by recurrent exacerbations despite being on high dose ICS and sometimes oral corticosteroids, with a high blood eosinophil count and a raised level of nitric oxide in exhaled breath. This phenotype has been associated with a Type-2 (T2) inflammatory profile with expression of interleukin (IL)-4, IL-5, and IL-13. Molecular phenotyping has also revealed non-T2 inflammatory phenotypes such as Type-1 or Type-17 driven phenotypes. Antibody treatments targeted at the T2 targets such as anti-IL5, anti-IL5Rα, and anti-IL4Rα antibodies are now available for treating severe eosinophilic asthma, in addition to anti-immunoglobulin E antibody for severe allergic asthma. No targeted treatments are currently available for non-T2 inflammatory phenotypes. Long-term azithromycin and bronchial thermoplasty may be considered. The future lies with molecular phenotyping of the airway inflammatory process to refine asthma endotypes for precision medicine.
Copyright © 2022 The Chinese Medical Association, produced by Wolters Kluwer, Inc. under the CC-BY-NC-ND license.
Conflict of interest statement
KFC has received honoraria for participating in Advisory Board meetings of GSK, AstraZeneca, Roche, Novartis, Merck, Boehringer Ingelheim, TEVA and Shionogi regarding treatments for asthma, chronic obstructive pulmonary disease and chronic cough and has also been renumerated for speaking engagements. PHP has received honoraria for participating in Advisory Board meetings of GSK and AstraZeneca, regarding treatments for asthma and has also been remunerated for speaking engagements. Other authors have no conflicts of interest to declare.
Figures
References
-
- Huang K, Yang T, Xu J, Yang L, Zhao J, Zhang X, et al. . Prevalence, risk factors, and management of asthma in China: a national cross-sectional study. Lancet 2019; 394:407–418. doi: 10.1016/s0140-6736(19)31147-x. - PubMed
-
- Hekking PP, Wener RR, Amelink M, Zwinderman AH, Bouvy ML, Bel EH. The prevalence of severe refractory asthma. J Allergy Clin Immunol 2015; 135:896–902. doi: 10.1016/j.jaci.2014.08.042. - PubMed
-
- Backman H, Jansson SA, Stridsman C, Eriksson B, Hedman L, Eklund BM, et al. . Severe asthma - a population study perspective. Clin Exp Allergy 2019; 49:819–828. doi: 10.1111/cea.13378. - PubMed
-
- Su N, Lin JT, Wang WY, Chen P, Zhou X, Wan HY, et al. . A crosssection study of severe asthma in eight provinces of China (in Chinese). Zhonghua Nei Ke Za Zhi 2016; 55:917–921. doi: 10.3760/cma.j. issn.0578-1426.2016.12.002. - PubMed
-
- Wang WY, Lin JT, Zhou X, Chen P, Wan HY, Yin KS, et al. . A survey on clinical characteristics and risk factors of severe asthma in China (in Chinese). Zhonghua Yi Xue Za Zhi 2020; 100:1106–1111. doi: 10.3760/cma.j.cn112137-20191117-02497. - PubMed
