

Facial Fractures Have Similar Outcomes When Managed by Either Otolaryngology or Plastic Surgery: Encounters From a Single Level I Trauma Center
- PMID: 35633765
- PMCID: PMC9133515
- DOI: 10.1177/19433875211020615
Facial Fractures Have Similar Outcomes When Managed by Either Otolaryngology or Plastic Surgery: Encounters From a Single Level I Trauma Center
Abstract
Study design: Retrospective cohort.
Objective: Traumatic facial fractures (FFs) often require specialty consultation with Plastic Surgery (PS) or Otolaryngology (ENT); however, referral patterns are often non-standardized and institution specific. Therefore, we sought to compare management patterns and outcomes between PS and ENT, hypothesizing no difference in operative rates, complications, or mortality.
Methods: We performed a retrospective analysis of patients with FFs at a single Level I trauma center from 2014 to 2017. Patients were compared by consulting service: PS vs. ENT. Chi-square and Mann-Whitney-U tests were performed.
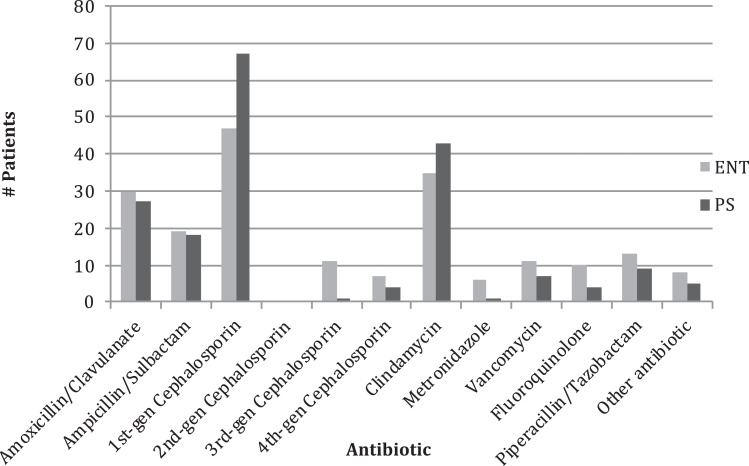
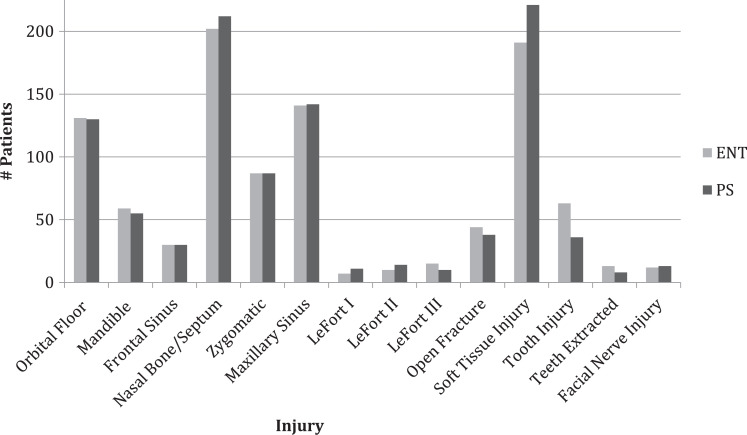
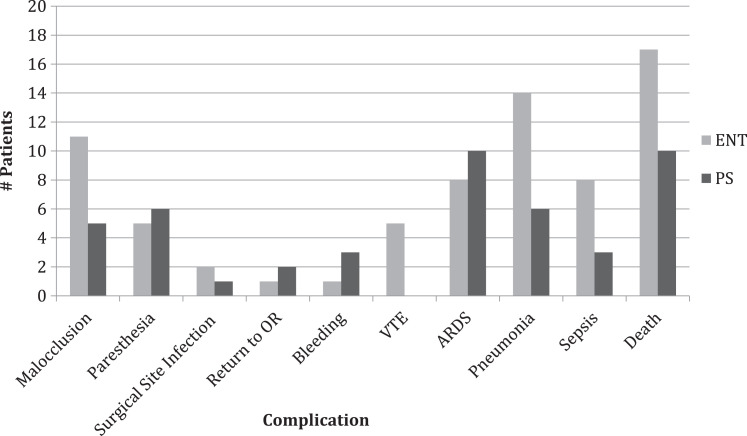
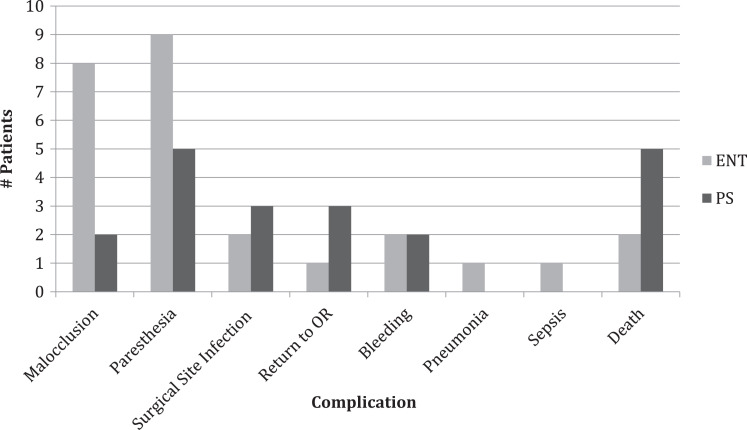
Results: Of the 755 patients with FFs, 378 were consulted by PS and 377 by ENT. There was no difference in demographic data (P > 0.05). Patients managed by ENT received a longer mean course of antibiotics (9.4 vs 7.0 days, P = 0.008) and had a lower rate of open reduction internal fixation (ORIF) (9.8% vs. 15.3%, P = 0.017), compared to PS patients. No difference was observed in overall operative rate (15.1% vs. 19.8%), use of computed tomography (CT) imaging (99% vs. 99%), time to surgery (65 vs. 55 hours, P = 0.198), length of stay (LOS) (4 vs. 4 days), 30-day complication rate (10.6% vs. 7.1%), or mortality (4.5% vs. 2.6%) (all P > 0.05).
Conclusion: Our study demonstrated similar baseline characteristics, operative rates, complications, and mortality between FFs patients who had consultation by ENT and PS. This supports the practice of allowing both ENT and PS to care for trauma FFs patients, as there appears to be similar standardized care and outcomes. Future studies are needed to evaluate the generalizability of our findings.
Keywords: antibiotics; facial fracture; facial trauma; otolaryngology; plastic surgery.
© The Author(s) 2021.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Allareddy V, Allareddy V, Nalliah RP. Epidemiology of facial fracture injuries. J Oral Maxillofac Surg. 2011;69(10):2613–2618. - PubMed
-
- Chukwulebe S, Hogrefe C. The diagnosis and management of facial bone fractures. Emerg Med Clin North Am. 2019;37(1):137–151. - PubMed
-
- Baylan JM, Jupiter D, Parker WL, Czerwinski M. Management of zygomatic fractures: a national survey. J Craniofac Surg. 2016;27(6):1571–1575. - PubMed
-
- Susarla SM, Mundinger GS, O’Brien-Coon D, et al. Does training background influence decision-making in the management of zygomaticomaxillary complex fractures? J Oral Maxillofac Surg. 2016;74(5):995–1012. - PubMed
-
- Bagheri SC, Dimassi M, Shahriari A, Khan HA, Jo C, Steed MB. Facial trauma coverage among level-1 trauma centers of the United States. J Oral Maxillofac Surg. 2008;66(5):963–967. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous