

Machine Learning Approach to Predicting Absence of Serious Bacterial Infection at PICU Admission
- PMID: 35634885
- PMCID: PMC10350635
- DOI: 10.1542/hpeds.2021-005998
Machine Learning Approach to Predicting Absence of Serious Bacterial Infection at PICU Admission
Abstract
Background and objectives: Serious bacterial infection (SBI) is common in the PICU. Antibiotics can mitigate associated morbidity and mortality but have associated adverse effects. Our objective is to develop machine learning models able to identify SBI-negative children and reduce unnecessary antibiotics.
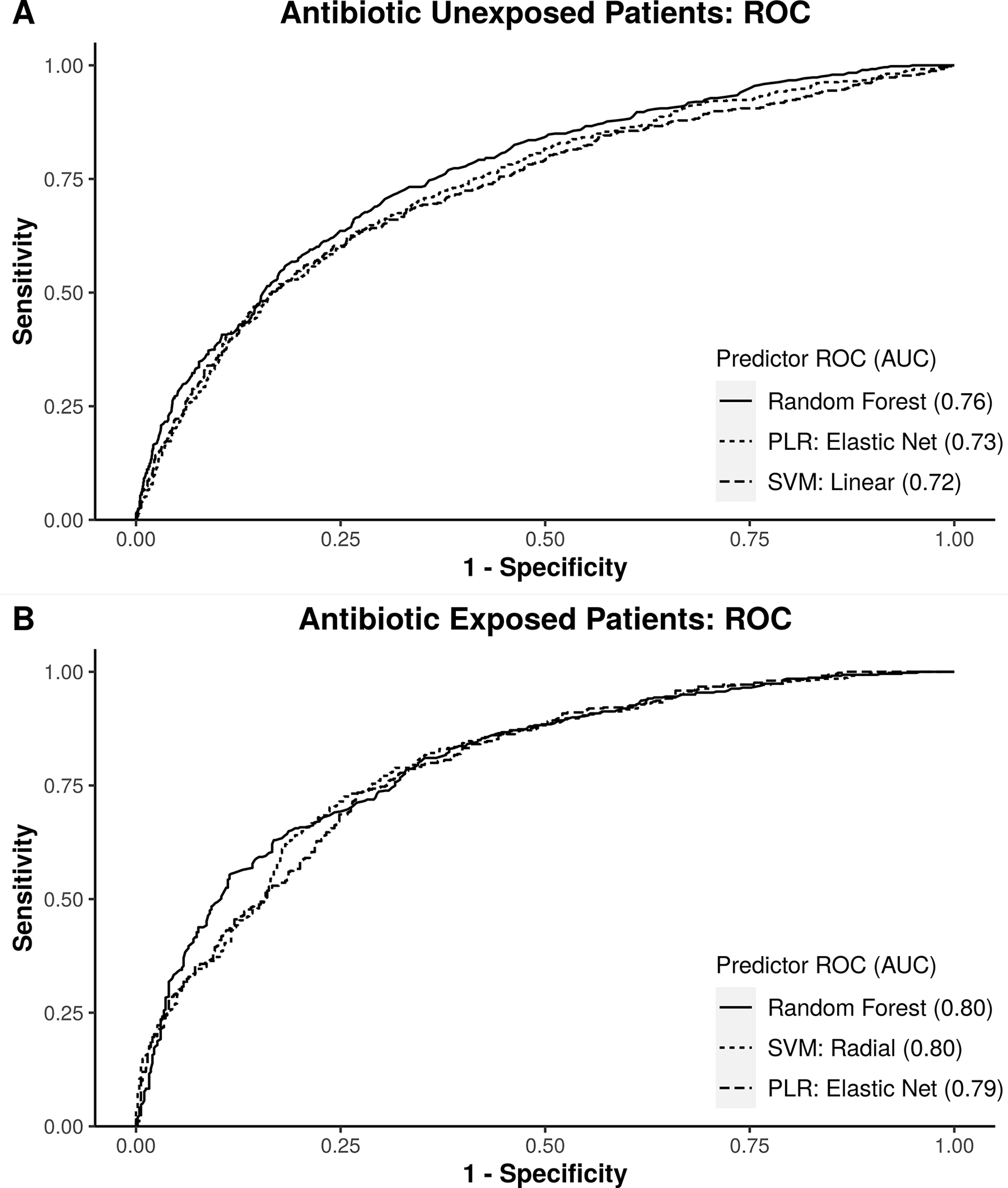
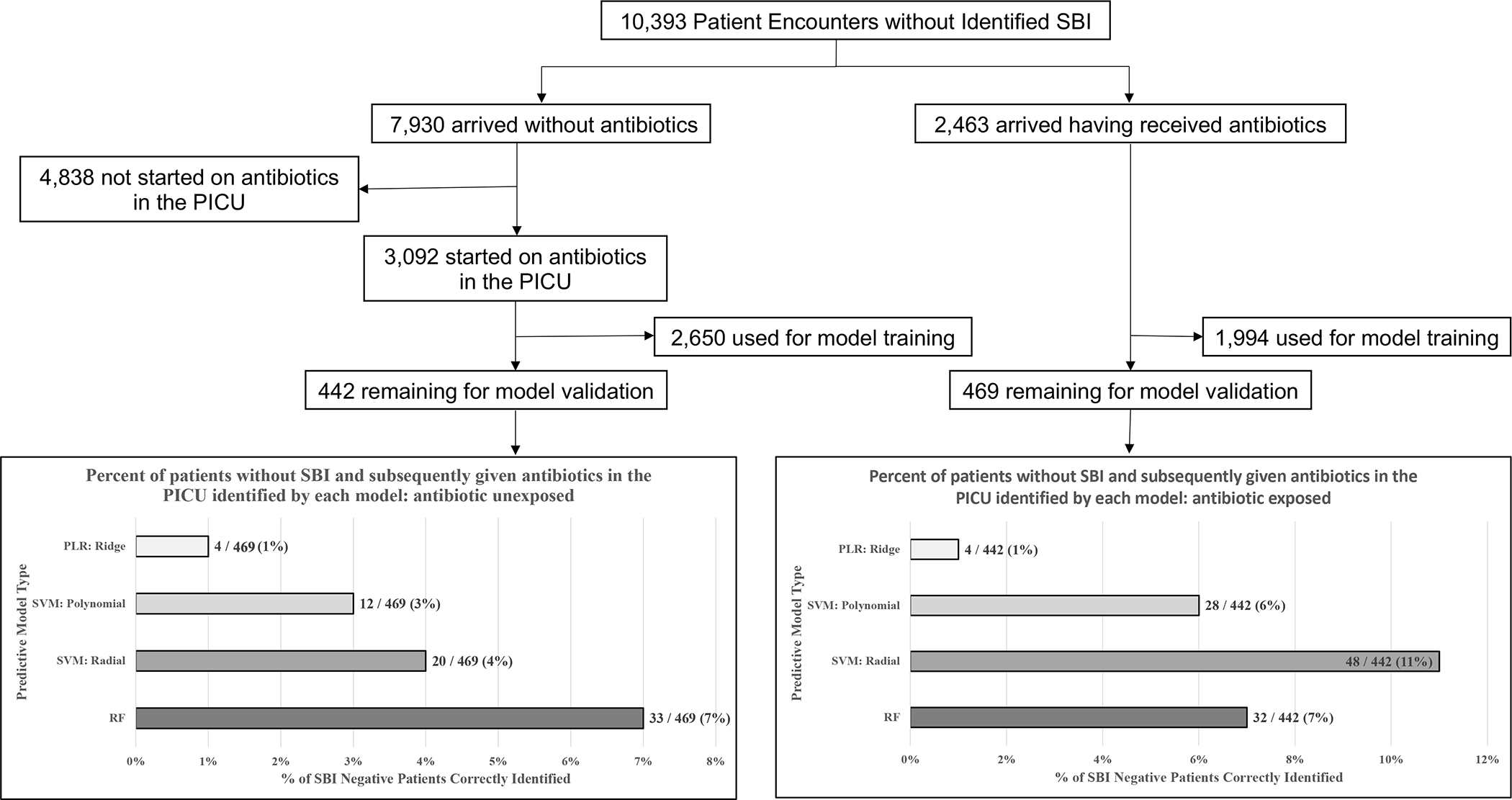
Methods: We developed models to predict SBI-negative status at PICU admission using vital sign, laboratory, and demographic variables. Children 3-months to 18-years-old admitted to our PICU, between 2011 and 2020, were included if evaluated for infection within 24-hours, stratified by documented antibiotic exposure in the 48-hours prior. Area under the receiver operating characteristic curve (AUROC) was the primary model accuracy measure; secondarily, we calculated the number of SBI-negative children subsequently provided antibiotics in the PICU identified as low-risk by each model.
Results: A total of 15 074 children met inclusion criteria; 4788 (32%) received antibiotics before PICU admission. Of these antibiotic-exposed patients, 2325 of 4788 (49%) had an SBI. Of the 10 286 antibiotic-unexposed patients, 2356 of 10 286 (23%) had an SBI. In antibiotic-exposed children, a radial support vector machine model had the highest AUROC (0.80) for evaluating SBI, identifying 48 of 442 (11%) SBI-negative children provided antibiotics in the PICU who could have been spared a median 3.7 (interquartile range 0.9-9.0) antibiotic-days per patient. In antibiotic-unexposed children, a random forest model performed best, but was less accurate overall (AUROC 0.76), identifying 33 of 469 (7%) SBI-negative children provided antibiotics in the PICU who could have been spared 1.1 (interquartile range 0.9-3.7) antibiotic-days per patient.
Conclusions: Among children who received antibiotics before PICU admission, machine learning models can identify children at low risk of SBI and potentially reduce antibiotic exposure.
Copyright © 2022 by the American Academy of Pediatrics.
Conflict of interest statement
Figures
Similar articles
-
PROGNOSTIC ACCURACY OF MACHINE LEARNING MODELS FOR IN-HOSPITAL MORTALITY AMONG CHILDREN WITH PHOENIX SEPSIS ADMITTED TO THE PEDIATRIC INTENSIVE CARE UNIT.Shock. 2025 Jan 1;63(1):80-87. doi: 10.1097/SHK.0000000000002501. Shock. 2025. PMID: 39671551
-
Procalcitonin to Detect Bacterial Infections in Critically Ill Pediatric Patients.Clin Pediatr (Phila). 2017 Aug;56(9):821-827. doi: 10.1177/0009922817715937. Clin Pediatr (Phila). 2017. PMID: 28720036
-
Machine learning-based prediction of delirium 24 h after pediatric intensive care unit admission in critically ill children: A prospective cohort study.Int J Nurs Stud. 2023 Oct;146:104565. doi: 10.1016/j.ijnurstu.2023.104565. Epub 2023 Jul 16. Int J Nurs Stud. 2023. PMID: 37542959
-
Predicting long-term neurocognitive outcome after pediatric intensive care unit admission for bronchiolitis-preliminary exploration of the potential of machine learning.Eur J Pediatr. 2024 Jan;183(1):471-482. doi: 10.1007/s00431-023-05307-3. Epub 2023 Nov 6. Eur J Pediatr. 2024. PMID: 37930398 Free PMC article.
-
[Management of children with fever without localizing signs of an infection].Arch Pediatr. 2001 Mar;8(3):324-30. Arch Pediatr. 2001. PMID: 11270261 Review. French.
Cited by
-
Navigating Complexity: Enhancing Pediatric Diagnostics With Large Language Models.Pediatr Crit Care Med. 2024 Jun 1;25(6):577-580. doi: 10.1097/PCC.0000000000003483. Epub 2024 Jun 5. Pediatr Crit Care Med. 2024. PMID: 38836714 Free PMC article. No abstract available.
-
Serum lactate is associated with increased illness severity in immunocompromised pediatric hematology oncology patients presenting to the emergency department with fever.Front Oncol. 2022 Oct 6;12:990279. doi: 10.3389/fonc.2022.990279. eCollection 2022. Front Oncol. 2022. PMID: 36276165 Free PMC article.
-
Development of a Pediatric Blood Pressure Percentile Tool for Clinical Decision Support.JAMA Netw Open. 2022 Oct 3;5(10):e2236918. doi: 10.1001/jamanetworkopen.2022.36918. JAMA Netw Open. 2022. PMID: 36251296 Free PMC article.
-
Diagnostic Stewardship of Blood Cultures in the Pediatric ICU Using Machine Learning.Hosp Pediatr. 2025 Jun 1;15(6):e240-e244. doi: 10.1542/hpeds.2024-008235. Hosp Pediatr. 2025. PMID: 40398877 Free PMC article.
-
Focused review on artificial intelligence for disease detection in infants.Front Digit Health. 2024 Nov 25;6:1459640. doi: 10.3389/fdgth.2024.1459640. eCollection 2024. Front Digit Health. 2024. PMID: 39654981 Free PMC article. Review.
References
-
- Brindha SM, Jayashree M, Singhi S, Taneja N. Study of nosocomial urinary tract infections in a pediatric intensive care unit. J Trop Pediatr. 2011;57(5):357–362. - PubMed
-
- Delport SD, Brisley T. Aetiology and outcome of severe community-acquired pneumonia in children admitted to a paediatric intensive care unit. S Afr Med J. 2002;92(11):907–911. - PubMed
-
- Gray J, Gossain S, Morris K. Three-year survey of bacteremia and fungemia in a pediatric intensive care unit. Pediatr Infect Dis J. 2001;20(4):416–421. - PubMed
-
- Maldini B, Antolic S, Sakic-Zdravcevic K, Karaman-Ilic M, Jankovic S. Evaluation of bacteremia in a pediatric intensive care unit: epidemiology, microbiology, sources sites and risk factors. Coll Antropol. 2007;31(4):1083–1088. - PubMed
-
- Mathot F, Duke T, Daley AJ, Butcher T. Bacteremia and pneumonia in a tertiary PICU: an 11-year study. Pediatr Crit Care Med. 2015;16(2):104–113. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
