

Bacterial etiology and mortality rate in community-acquired pneumonia, healthcare-associated pneumonia and hospital-acquired pneumonia in Thai university hospital
- PMID: 35637232
- PMCID: PMC9150030
- DOI: 10.1038/s41598-022-12904-z
Bacterial etiology and mortality rate in community-acquired pneumonia, healthcare-associated pneumonia and hospital-acquired pneumonia in Thai university hospital
Abstract
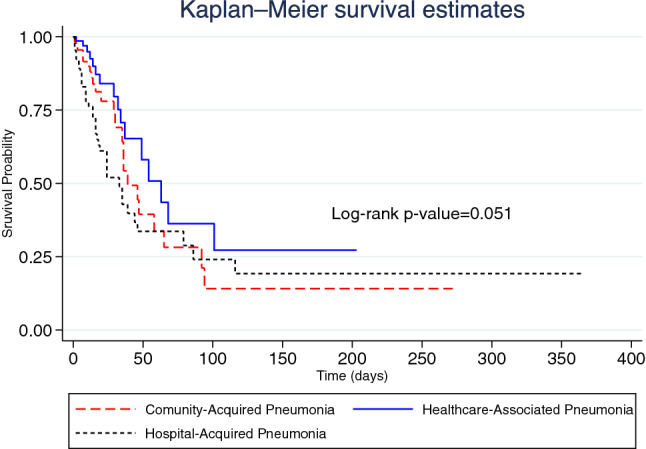
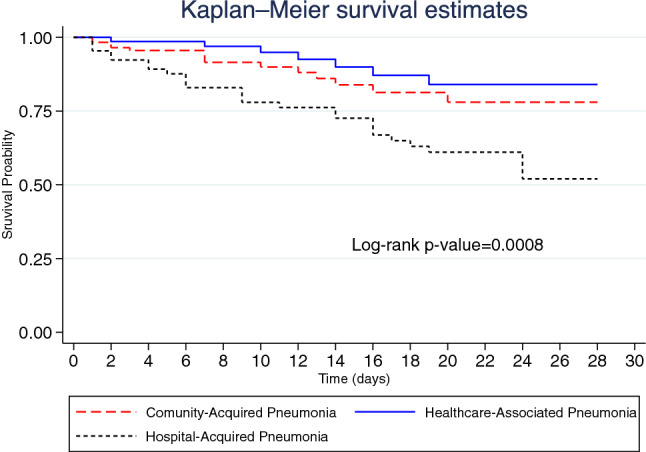
Pneumonia is caused by infection at the pulmonary parenchyma which constitutes a crucial risk factor for morbidity and mortality. We aimed to determine the mortality rate and its risk factors as well as etiology among inpatients with community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP) and healthcare-associated pneumonia (HCAP). A hospital-based retrospective cohort study was conducted in a university hospital located in Bangkok, Thailand. A total of 250 inpatients with pneumonia was included in the present study. The inhospital mortality rate was 1.25 (95% CI 0.99-1.56) per 100 person-days. The present study reported that overall pneumonia caused by gram-negative pathogens accounted for 60.5%. P. aeruginosa was a frequent gram-negative pathogen among these participants, especially among patients with HCAP and HAP. Adjusted hazard ratio (AHR) of inhospital mortality among patients with HAP was 1.75 (95% CI 1.01-3.03) times that of those among patients with CAP, while AHR for 28-day mortality among patients with HAP compared with those with CAP was 2.81 (95% CI 1.38-5.75). Individual risks factors including cardiomyopathy, active-smoker and insulin use were potential risk factors for mortality. Initial qSOFA and acid-based disturbance should be assessed to improve proper management and outcomes.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Mandell, L. A. et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 44 (2007). - PubMed
-
- Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respirat. Crit. Care Med. 171 (2005). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
