

Mortality-causing mechanisms and healthcare resource utilisation of treatment-resistant depression: A six-year population-based cohort study
- PMID: 35637863
- PMCID: PMC9142753
- DOI: 10.1016/j.lanwpc.2022.100426
Mortality-causing mechanisms and healthcare resource utilisation of treatment-resistant depression: A six-year population-based cohort study
Abstract
Background: Few studies investigated the mechanisms of treatment-resistant depression (TRD) leading to the worsened survival outcome, and economic evidence was mostly restricted to short follow-ups. We aimed to examine the association and potential mediators between TRD and all-cause mortality, and estimate a longer-term associated health resource utilisation pattern.
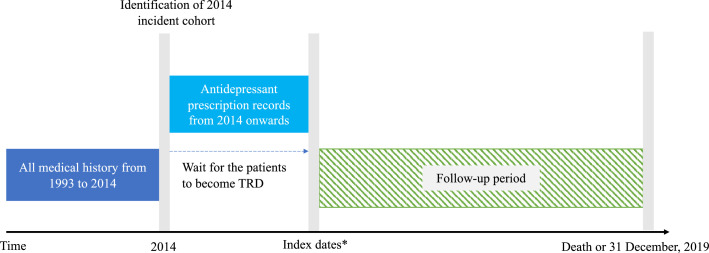
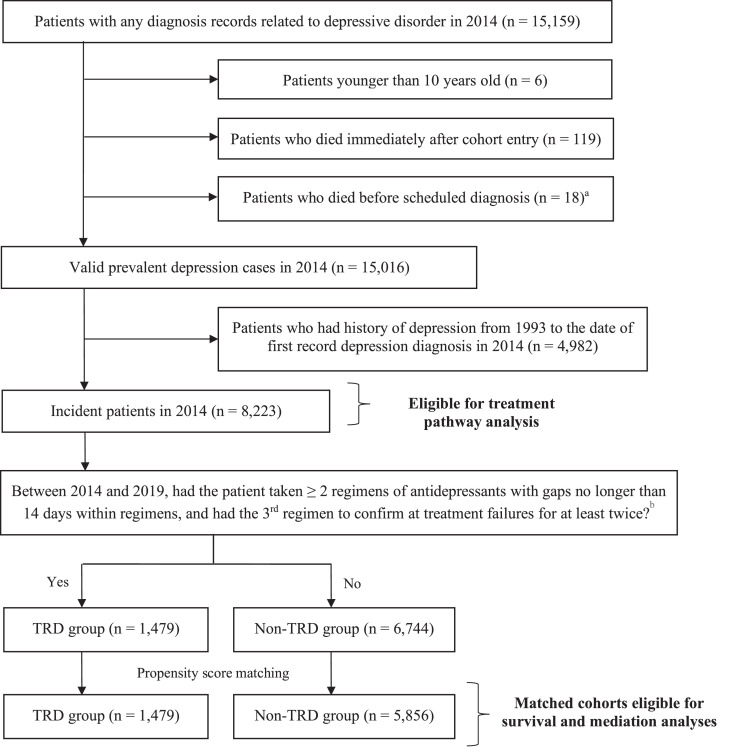
Methods: This was a population-based cohort study using territory-wide electronic medical records in Hong Kong. Incident depression patients diagnosed in 2014 were followed up from the first diagnosis to death or December 2019 for TRD identification. We matched the TRD cohort 1:4 to the non-TRD cohort on propensity scores estimated by age, sex, history of physical disorders, and history of psychiatric conditions before depression diagnoses.
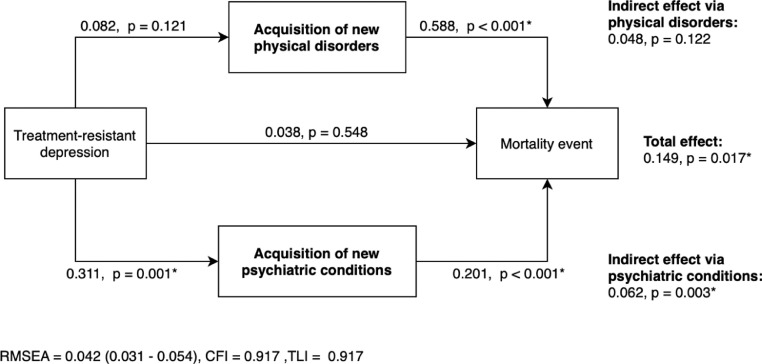
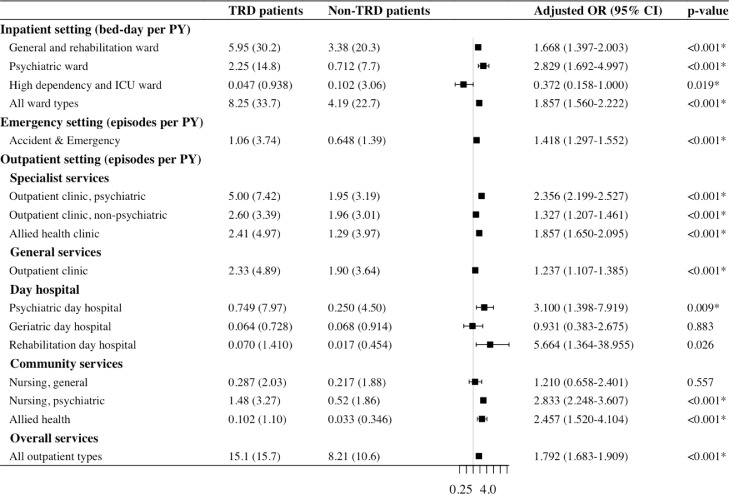
Findings: 18% of incident patients developed TRD within six years of follow-up. Cox model showed that patients with TRD had 1⋅52-fold (95% CI: 1⋅14-2⋅02) greater risk of all-cause mortality, compared with non-TRD patients. Path analysis suggested that post-TRD psychiatric conditions significantly mediated 41⋅6% of mortality in patients with TRD (p=0.003). TRD was associated with 1⋅8-fold (95%CI: 1⋅63-2⋅00) higher healthcare costs compared to non-TRD patients over six years in negative binomial regression, with higher costs for both psychiatric and non-psychiatric services utilisation in all settings.
Interpretation: Identifying patients with TRD and subsequent monitoring for post-TRD psychiatric diagnoses could be a way to reduce premature mortality. Multidisciplinary care involving both psychiatric and general medical professionals is also warranted to relieve the multifaceted impacts on healthcare resources and overall cost.
Funding: Unconditional educational grant from Janssen.
Keywords: Death-causing mechanism; Health Economics; Mediation analysis; Population-based electronic medical records; Restrospective cohort study; Treatment-resistant depression.
© 2022 The Authors.
Conflict of interest statement
X Li received research grants from Research Fund Secretariat of the Food and Health Bureau (HMRF, HKSAR), Research Grants Council Early Career Scheme (RGC/ECS, HKSAR), Janssen and Pfizer; internal funding from the University of Hong Kong; consultancy fee from Merck Sharp & Dohme, unrelated to this work; H Luo received research grants Research Grants Council Early Career Scheme (RGC/ECS, HKSAR) unrelated to this work. S Chan received research support from GRF, Research Grant Council; HMRF, Food and Health Bureau. FTT Lai was supported by the RGC Postdoctoral Fellowship 2020/21 (inaugural exercise) funded by the Research Grants Council, University Grants Committee, Hong Kong SAR. J F Hayes was supported by the Wellcome Trust (211085/Z/18/Z), University College London Hospitals NIHR Biomedical Research Centre and the NIHR ARC North Thames Academy. He received consultancy fees from the Wellcome Trust and Juli Health, unrelated to this work. P Ip received research grants from Research Fund Secretariat of the Food and Health Bureau (HMRF, HKSAR), Research Grants Council (GRF and CRF, HKSAR) and project grant from the Hong Kong Jockey Club Charities Trust. EWY Chan received honorarium from the Hospital Authority, research grants from Innovation and Technology Commission of HKSAR, Narcotics Division of the Security Bureau of HKSAR, National Health and Medical Research Council (NHMRC, Australia), National Natural Science Foundation of China (NSFC), Research Fund Secretariat of the Food and Health Bureau (HMRF, HKSAR), Research Grants Council (RGC, HKSAR), Wellcome Trust; Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Janssen, Pfizer, RGA, Takeda and Novartis, and consultancy fee from Novartis outside the submitted work. She is also the President of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR), Hong Kong Regional Chapter. ICK Wong received research funding outside the submitted work from Amgen, Bristol-Myers Squibb, Pfizer, Janssen, Bayer, GSK, Novartis, Takeda, the Hong Kong RGC, and the Hong Kong Health and Medical Research Fund, National Institute for Health Research in England, European Commission, National Health and Medical Research Council in Australia, and has also received speaker fees from Janssen and Medice over the past three years. He is also an independent non-executive director of Jacobson Medical in Hong Kong.
Figures
References
-
- World Health Organisation . World Health Organisation; Geneva: 2017. Depression and Other Common Mental Disorders: Global Health Estimates.
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. - PMC - PubMed
-
- Liu Q., He H., Yang J., Feng X., Zhao F., Lyu J. Changes in the global burden of depression from 1990 to 2017: Findings from the Global Burden of Disease study. J Psychiatry Res. 2020;126:134–140. - PubMed
-
- Fava M., Davidson K.G. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am. 1996;19(2):179–200. - PubMed
-
- Trevino K., McClintock S.M., McDonald Fischer N., Vora A., Husain M.M. Defining treatment-resistant depression: a comprehensive review of the literature. Ann Clin Psychiatry. 2014;26(3):222–232. - PubMed
LinkOut - more resources
Full Text Sources
