

Ophthalmological Manifestations of Oculocutaneous and Ocular Albinism: Current Perspectives
- PMID: 35637898
- PMCID: PMC9148211
- DOI: 10.2147/OPTH.S329282
Ophthalmological Manifestations of Oculocutaneous and Ocular Albinism: Current Perspectives
Abstract
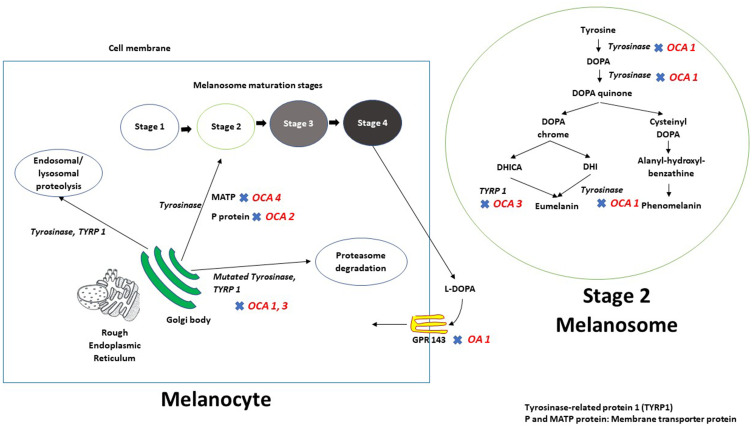
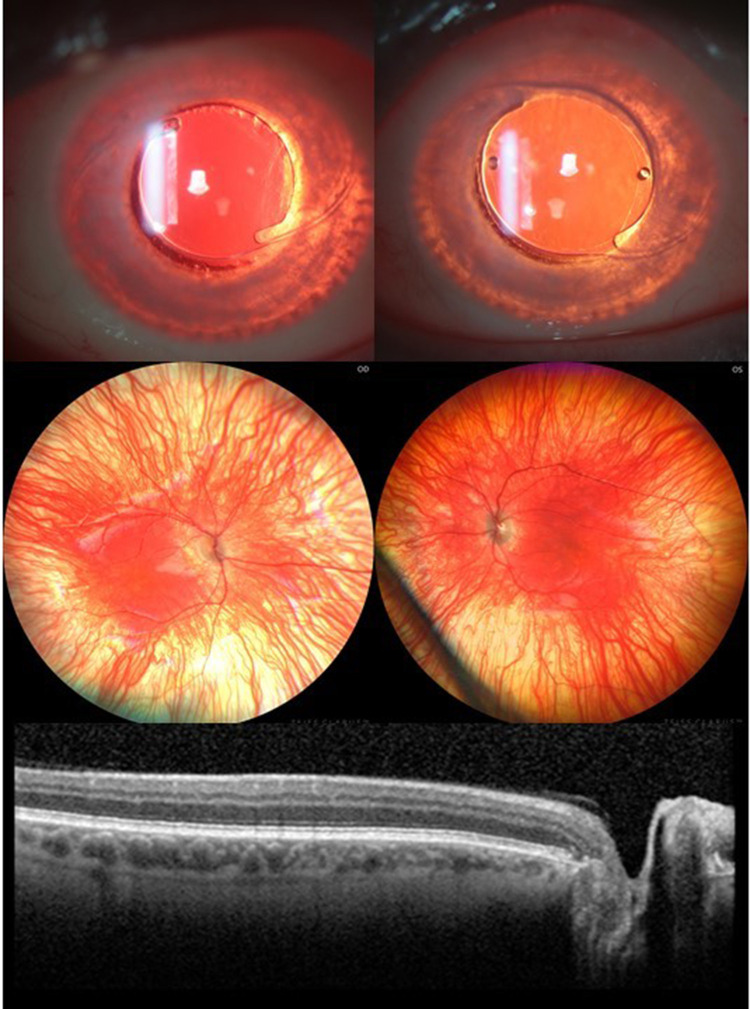
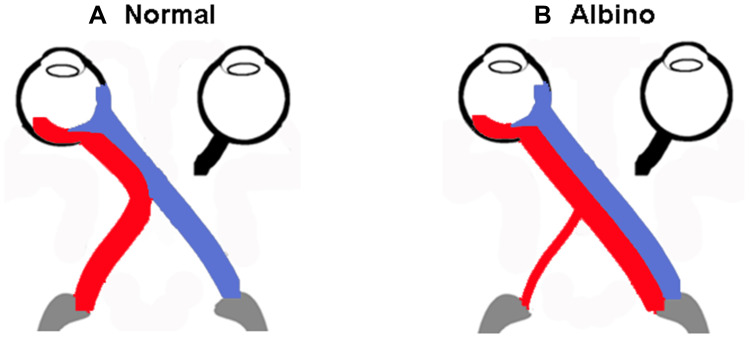
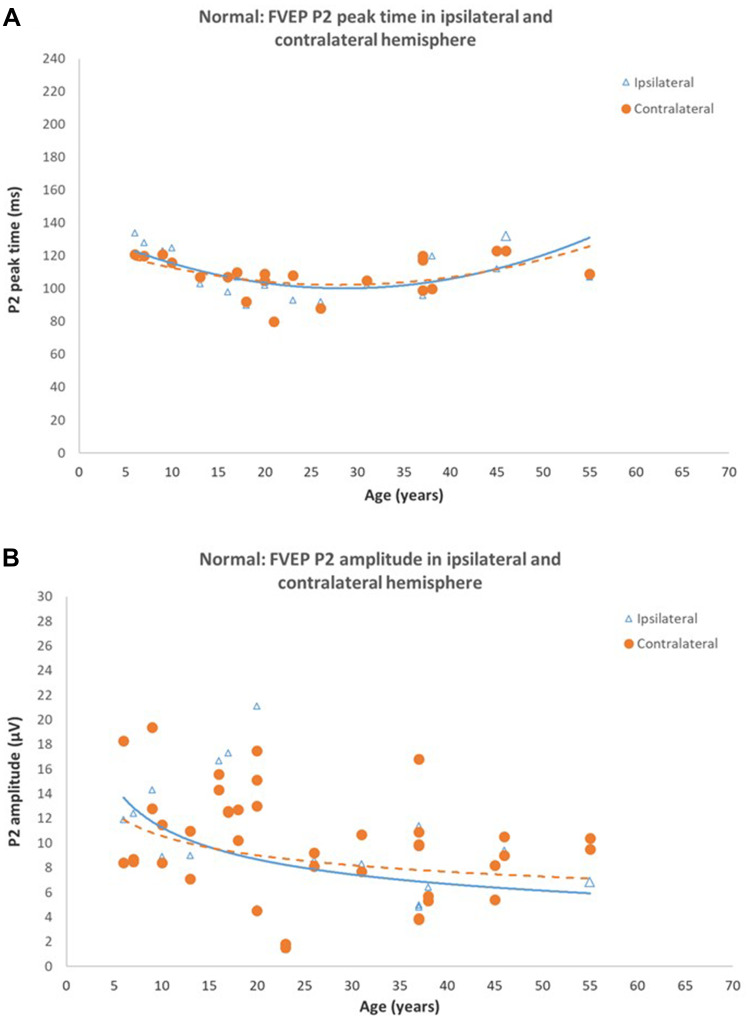
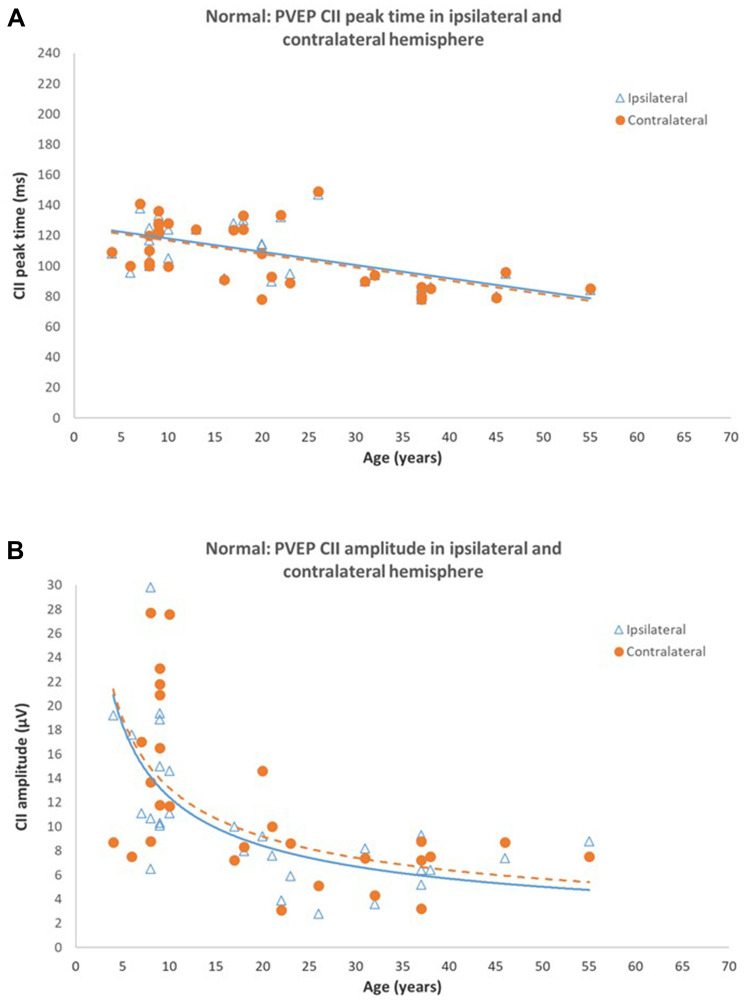
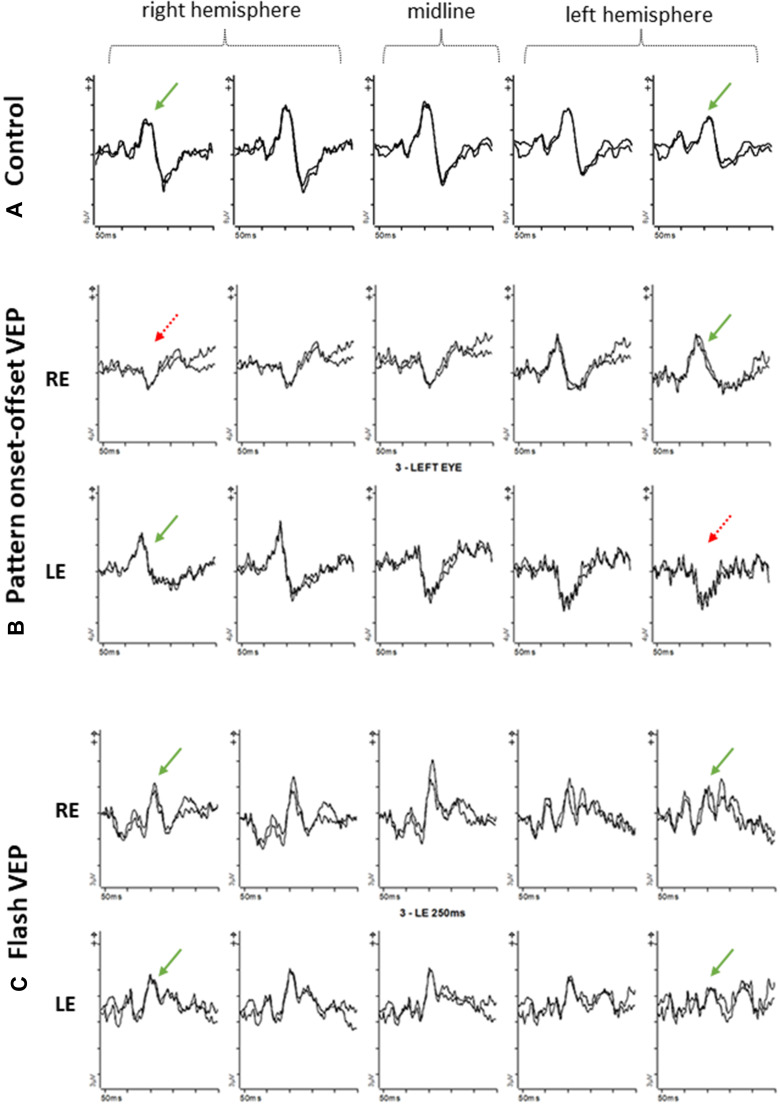
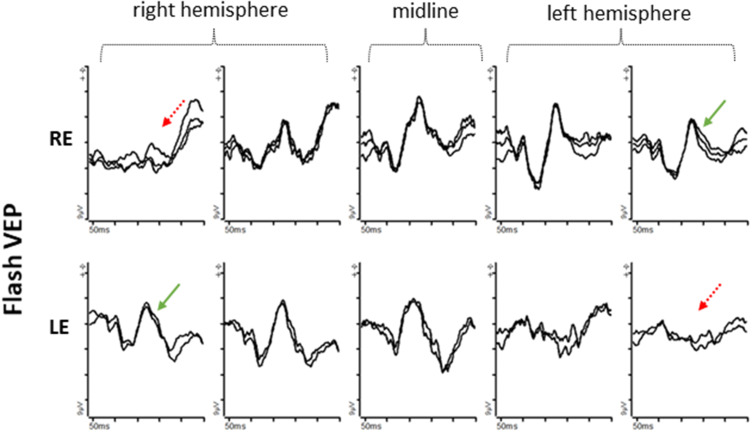
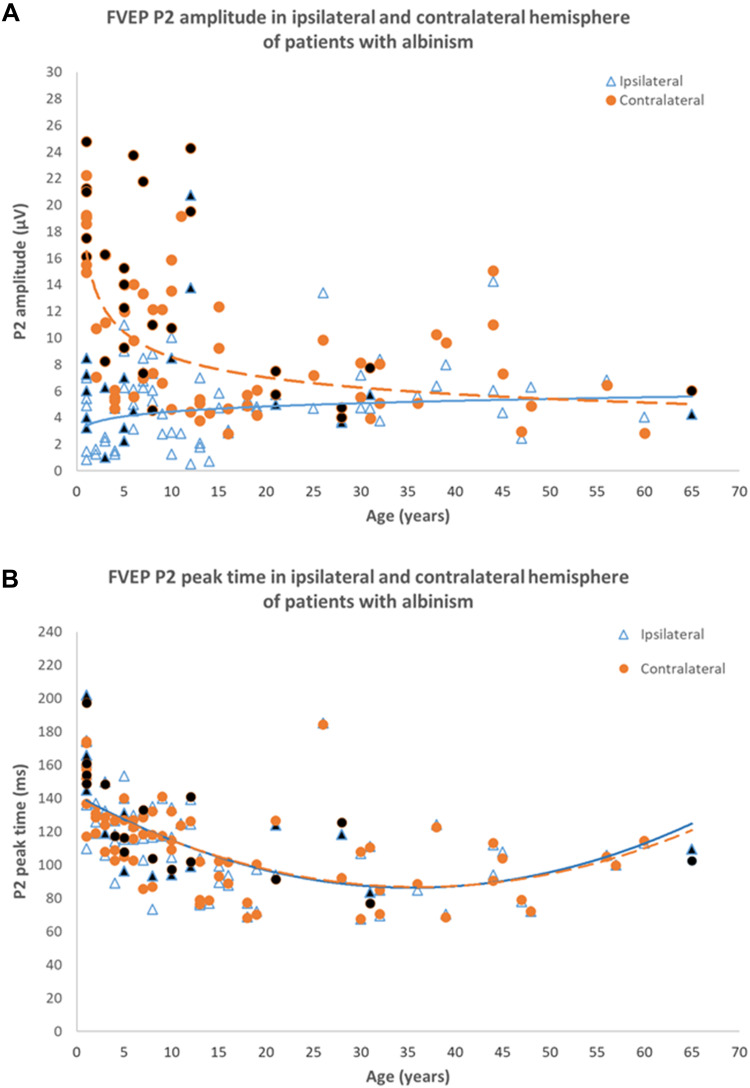
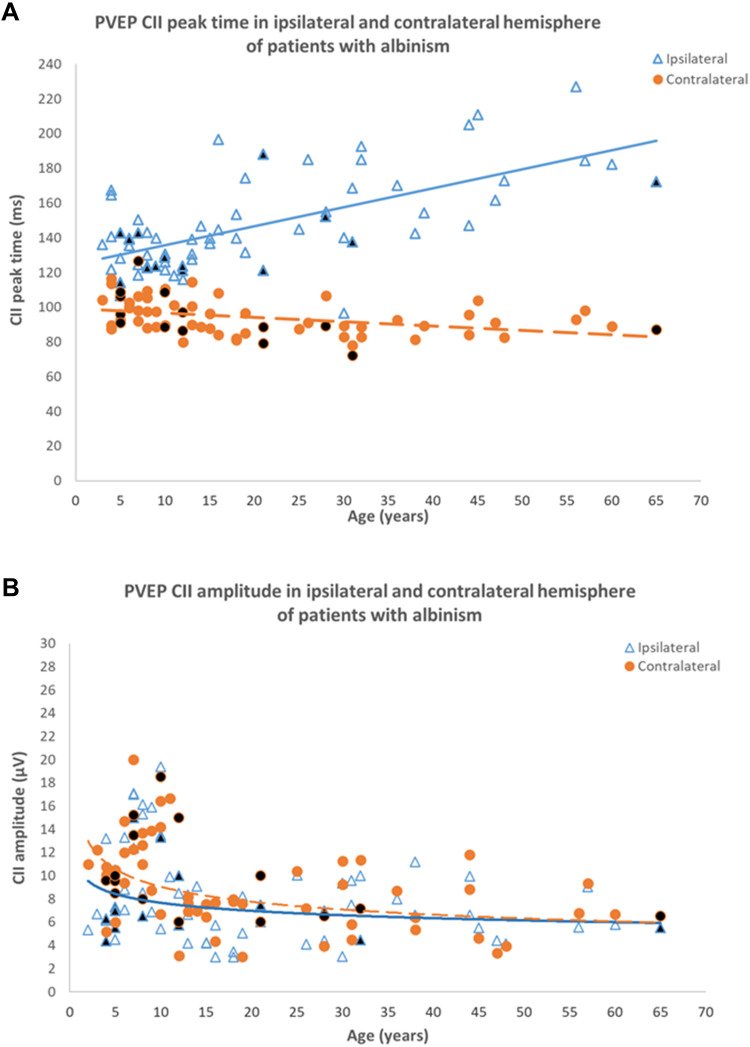
Albinism describes a heterogeneous group of genetically determined disorders characterized by disrupted synthesis of melanin and a range of developmental ocular abnormalities. The main ocular features common to both oculocutaneous albinism (OCA), and ocular albinism (OA) include reduced visual acuity, refractive errors, foveal hypoplasia, congenital nystagmus, iris and fundus hypopigmentation and visual pathway misrouting, but clinical signs vary and there is phenotypic overlap with other pathologies. This study reviews the prevalence, genetics and ocular manifestations of OCA and OA, including abnormal development of the optic chiasm. The role of visual electrophysiology in the detection of chiasmal dysfunction and visual pathway misrouting is emphasized, highlighting how age-associated changes in visual evoked potential (VEP) test results must be considered to enable accurate diagnosis, and illustrated further by the inclusion of novel VEP data in genetically confirmed cases. Differential diagnosis is considered in the context of suspected retinal and other disorders, including rare syndromes that may masquerade as albinism.
Keywords: VEP; albinism; foveal hypoplasia; misrouting; visual electrophysiology.
© 2022 Neveu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Marti A, Lasseaux E, Ezzedine K, et al. Lessons of a day hospital: comprehensive assessment of patients with albinism in a European setting. Pigment Cell Melanoma Res. 2018;31(2):318–329. - PubMed
-
- Manga P, Kerr R, Ramsay M, Kromberg JGR. Biology and genetics of oculocutaneous albinism and vitiligo-common pigmentation disorders in Southern Africa. S Afr Med J. 2013;103:984-988. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
