

Cup placement in primary total hip arthroplasty: how to get it right without navigation or robotics
- PMID: 35638598
- PMCID: PMC9257731
- DOI: 10.1530/EOR-22-0025
Cup placement in primary total hip arthroplasty: how to get it right without navigation or robotics
Abstract
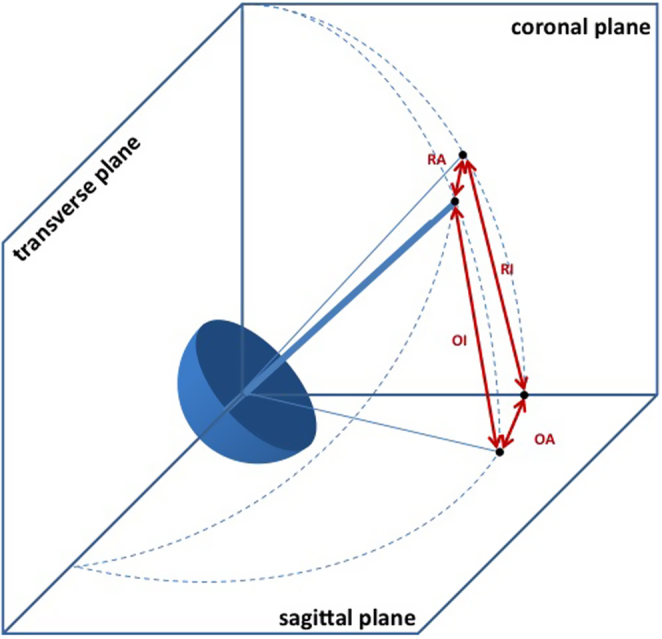
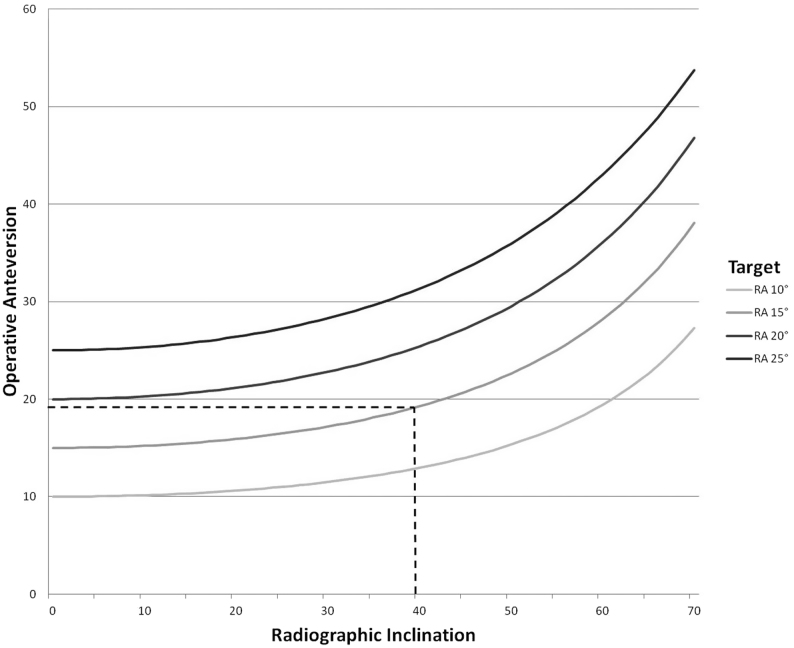
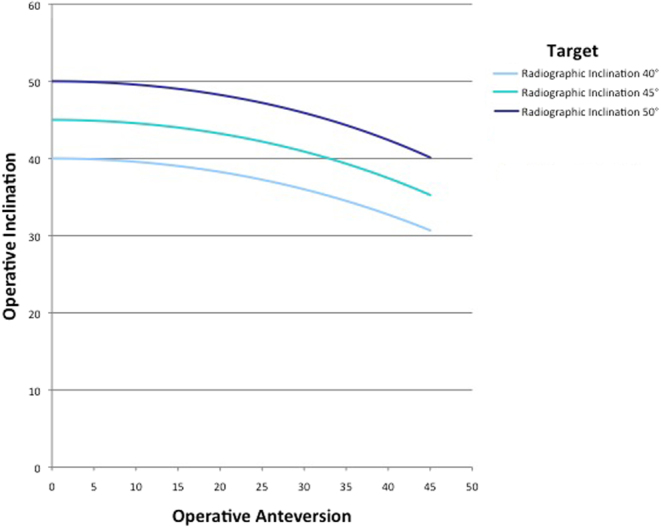
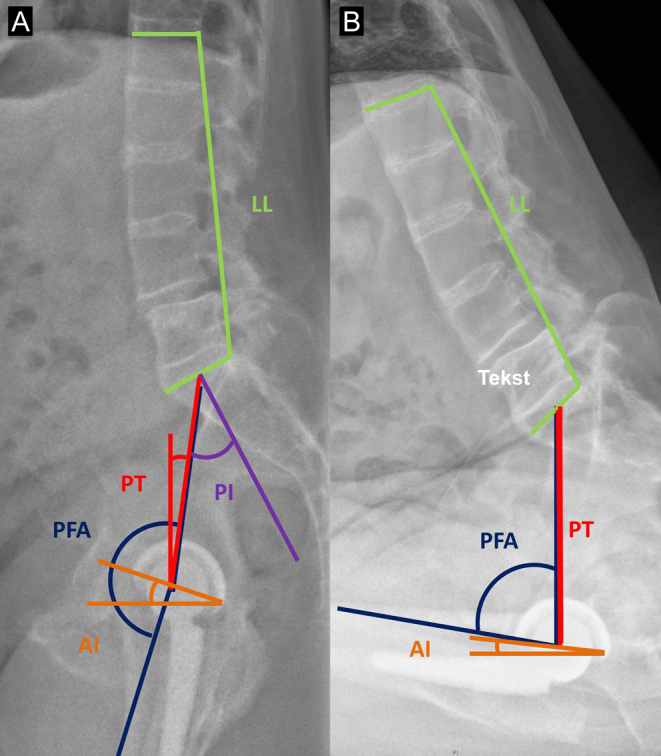
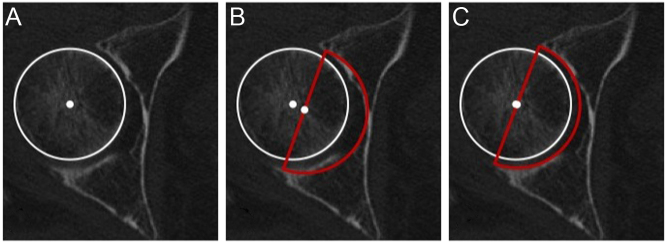
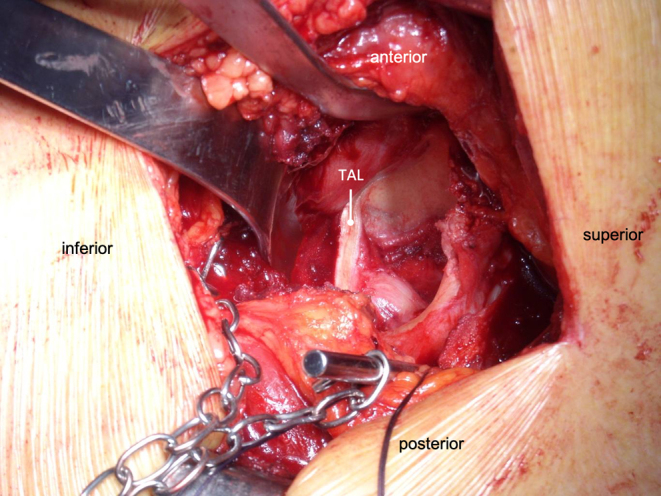
Acetabular component orientation and position are important factors in the short- and long-term outcomes of total hip arthroplasty. Different definitions of inclination and anteversion are used in the orthopaedic literature and surgeons should be aware of these differences and understand their relationships. There is no universal safe zone. Preoperative planning should be used to determine the optimum position and orientation of the cup and assess spinopelvic characteristics to adjust cup orientation accordingly. A peripheral reaming technique leads to a more accurate restoration of the centre of rotation with less variability compared with a standard reaming technique. Several intraoperative landmarks can be used to control the version of the cup, the most commonly used and studied is the transverse acetabular ligament. The use of an inclinometer reduces the variability associated with the use of freehand or mechanical alignment guides.
Keywords: cup; orientation; total hip.
Figures
References
-
- Al-Hajjar M, Leslie IJ, Tipper J, Williams S, Fisher J, Jennings LM. Effect of cup inclination angle during microseparation and rim loading on the wear of BIOLOX® delta ceramic-on-ceramic total hip replacement. Journal of Biomedical Materials Research: Part B, Applied Biomaterials 201095263–268. ( 10.1002/jbm.b.31708) - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
