

SARS-CoV-2 transmission, persistence of immunity, and estimates of Omicron's impact in South African population cohorts
- PMID: 35638937
- PMCID: PMC9161370
- DOI: 10.1126/scitranslmed.abo7081
SARS-CoV-2 transmission, persistence of immunity, and estimates of Omicron's impact in South African population cohorts
Abstract
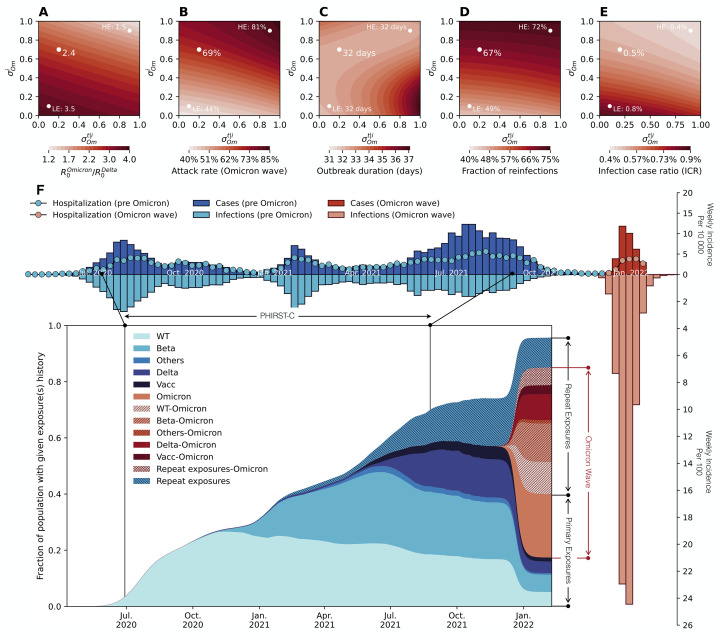
Understanding the build-up of immunity with successive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants and the epidemiological conditions that favor rapidly expanding epidemics will help facilitate future pandemic control. We analyzed high-resolution infection and serology data from two longitudinal household cohorts in South Africa to reveal high cumulative infection rates and durable cross-protective immunity conferred by prior infection in the pre-Omicron era. Building on the history of past exposures to different SARS-CoV-2 variants and vaccination in the cohort most representative of South Africa's high urbanization rate, we used mathematical models to explore the fitness advantage of the Omicron variant and its epidemic trajectory. Modeling suggests that the Omicron wave likely infected a large fraction (44 to 81%) of the population, leaving a complex landscape of population immunity primed and boosted with antigenically distinct variants. We project that future SARS-CoV-2 resurgences are likely under a range of scenarios of viral characteristics, population contacts, and residual cross-protection.
Figures
References
-
- Buss L. F., Prete C. A. Jr., Abrahim C. M. M., Mendrone A. Jr., Salomon T., de Almeida-Neto C., França R. F. O., Belotti M. C., Carvalho M. P. S. S., Costa A. G., Crispim M. A. E., Ferreira S. C., Fraiji N. A., Gurzenda S., Whittaker C., Kamaura L. T., Takecian P. L., da Silva Peixoto P., Oikawa M. K., Nishiya A. S., Rocha V., Salles N. A., de Souza Santos A. A., da Silva M. A., Custer B., Parag K. V., Barral-Netto M., Kraemer M. U. G., Pereira R. H. M., Pybus O. G., Busch M. P., Castro M. C., Dye C., Nascimento V. H., Faria N. R., Sabino E. C., Three-quarters attack rate of SARS-CoV-2 in the Brazilian Amazon during a largely unmitigated epidemic. Science 371, 288–292 (2021). 10.1126/science.abe9728 - DOI - PMC - PubMed
-
- Bhuiyan T. R., Hulse J. D., Hegde S. T., Akhtar M., Islam T., Khan Z. H., Khan I. I., Ahmed S., Rashid M., Rashid R., Gurley E. S., Shirin T., Khan A. I., Azman A. S., Qadri F., SARS-CoV-2 Seroprevalence before Delta Variant Surge, Chattogram, Bangladesh, March-June 2021. Emerg. Infect. Dis. 28, 429–431 (2022). 10.3201/eid2802.211689 - DOI - PMC - PubMed
-
- Huete-Pérez J. A., Ernst K. C., Cabezas-Robelo C., Páiz-Medina L., Silva S., Huete A., Prevalence and risk factors for SARS-CoV-2 infection in children with and without symptoms seeking care in Managua, Nicaragua: Results of a cross-sectional survey. BMJ Open 11, e051836 (2021). 10.1136/bmjopen-2021-051836 - DOI - PMC - PubMed
-
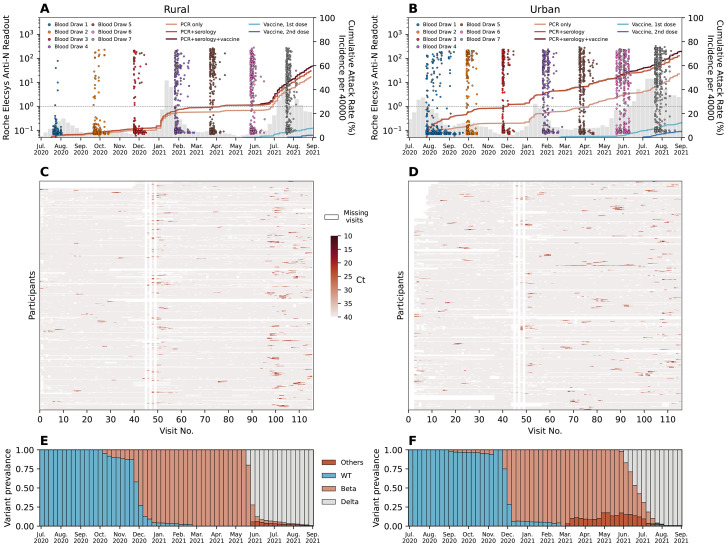
- Cohen C., Kleynhans J., von Gottberg A., McMorrow M. L., Wolter N., Bhiman J. N., Moyes J., du Plessis M., Carrim M., Buys A., Martinson N. A., Kahn K., Tollman S., Lebina L., Wafawanaka F., du Toit J. D., Gómez-Olivé F. X., Dawood F. S., Mkhencele T., Sun K., Viboud C., Tempia S.; PHIRST-C Group , SARS-CoV-2 incidence, transmission, and reinfection in a rural and an urban setting: Results of the PHIRST-C cohort study, South Africa, 2020-21. Lancet Infect. Dis. 22, 821–834 (2022). 10.1016/S1473-3099(22)00069-X - DOI - PMC - PubMed
-
- Tegally H., Wilkinson E., Lessells R. J., Giandhari J., Pillay S., Msomi N., Mlisana K., Bhiman J. N., von Gottberg A., Walaza S., Fonseca V., Allam M., Ismail A., Glass A. J., Engelbrecht S., Van Zyl G., Preiser W., Williamson C., Petruccione F., Sigal A., Gazy I., Hardie D., Hsiao N.-Y., Martin D., York D., Goedhals D., San E. J., Giovanetti M., Lourenço J., Alcantara L. C. J., de Oliveira T., Sixteen novel lineages of SARS-CoV-2 in South Africa. Nat. Med. 27, 440–446 (2021). 10.1038/s41591-021-01255-3 - DOI - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
