

Predictors of time to recovery and non-response during outpatient treatment of severe acute malnutrition
- PMID: 35639683
- PMCID: PMC9154090
- DOI: 10.1371/journal.pone.0267538
Predictors of time to recovery and non-response during outpatient treatment of severe acute malnutrition
Abstract
Background: Every year, over 4 million children are treated for severe acute malnutrition with varying program performance. This study sought to explore the predictors of time to recovery from and non-response to outpatient treatment of SAM.
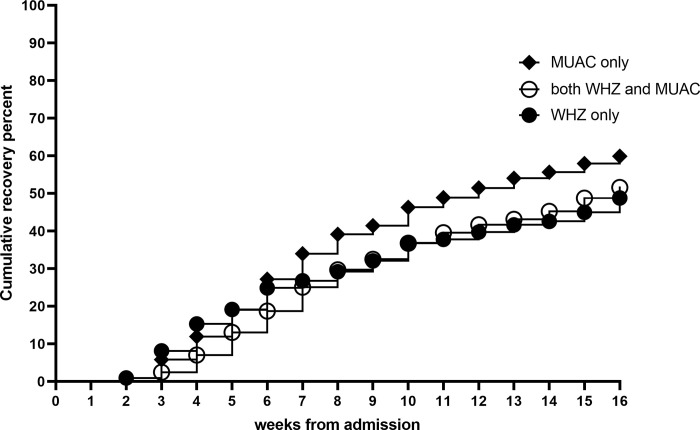
Methods: Children with weight-for-height z-score (WHZ) <-3 and/or mid-upper arm circumference (MUAC) <115 mm, without medical complications were enrolled in a trial (called MANGO) from outpatient clinics in Burkina Faso. Treatment included a weekly ration of ready-to-use therapeutic foods. Recovery was declared with WHZ ≥-2 and/or MUAC ≥125 mm, for two weeks without illness. Children not recovered by 16 weeks were considered as non-response to treatment. Predictors studied included admission characteristics, morbidity and compliance during treatment and household characteristics. Cox proportional hazard models were fitted and restricted mean time to recovery calculated. Logistic regression was used to analyse non-response to treatment.
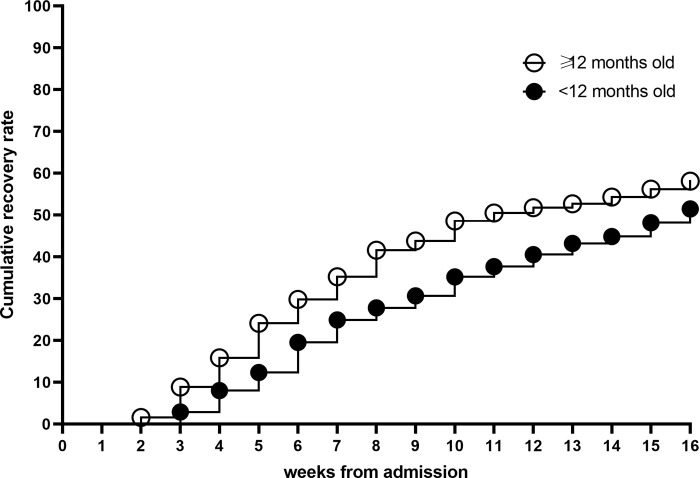
Results: Fifty-five percent of children recovered and mean time to recovery was eight weeks while 13% ended as non-response to treatment. Independent predictors of longer time to recovery or non-response included low age, being admitted with WHZ <-3, no illness nor anaemia at admission, illness episodes during treatment, skipped or missed visits, low maternal age and not practising open defecation. Eighty-four percent of children had at least one and 59% at least two illness episodes during treatment. This increased treatment duration by 1 to 4 weeks. Thirty-five percent of children missed at least one treatment visit. One missed visit predicted 3 weeks longer and two or more missed visits 5 weeks longer treatment duration.
Conclusions: Both longer time to recovery and higher non-response to treatment seem most strongly associated with illness episodes and missed visits during treatment. This indicates that prevention of illnesses would be key to shortening the treatment duration and that there is a need to seek ways to facilitate adherence.
Conflict of interest statement
STK was previously employed by Nutriset, a producer of RUTF. HF has received research grants from ARLA Food for Health Centre, and also has research collaboration with Nutriset. Other authors declare no financial relationships with any organisations that might have an interest in the submitted work in the previous five years, and declare no other relationships or activities that could appear to have influenced the submitted work. The declared competing interests do not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- World Health Organization, UNICEF. WHO child growth standards and the identification of severe acute malnutrition in infants and children: a joint statement by the World Health Organization and the United Nations Children’s Fund. [Internet]. 2009. [cited 2018 Mar 12]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK200775/ - PubMed
-
- United Nations Children’s Fund (UNICEF), World Health Organization, International, Bank for Reconstruction and Development/The World Bank. Levels and trends in child malnutrition: Key Findings of the 2020 Edition of the Joint Child Malnutrition Estimates. World Health Organization; 2020.
-
- Olofin I, McDonald CM, Ezzati M, Flaxman S, Black RE, Fawzi WW, et al.. Associations of Suboptimal Growth with All-Cause and Cause-Specific Mortality in Children under Five Years: A Pooled Analysis of Ten Prospective Studies. Wiley AS, editor. PLoS ONE. 2013. May 29;8(5):e64636. doi: 10.1371/journal.pone.0064636 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
