

Predictors of treatment response in a lupus nephritis population: lessons from the Aspreva Lupus Management Study (ALMS) trial
- PMID: 35640982
- PMCID: PMC9157342
- DOI: 10.1136/lupus-2021-000584
Predictors of treatment response in a lupus nephritis population: lessons from the Aspreva Lupus Management Study (ALMS) trial
Abstract
Objectives: To identify predictors of overall lupus and lupus nephritis (LN) responses in patients with LN.
Methods: Data from the Aspreva Lupus Management Study (ALMS) trial cohort was used to identify baseline predictors of response at 6 months. Endpoints were major clinical response (MCR), improvement, complete renal response (CRR) and partial renal response (PRR). Univariate and multivariate logistic regressions with least absolute shrinkage and selection operator (LASSO) and cross-validation in randomly split samples were utilised. Predictors were ranked by the percentage of times selected by LASSO and prediction performance was assessed by the area under the receiver operating characteristics (AUROC) curve.
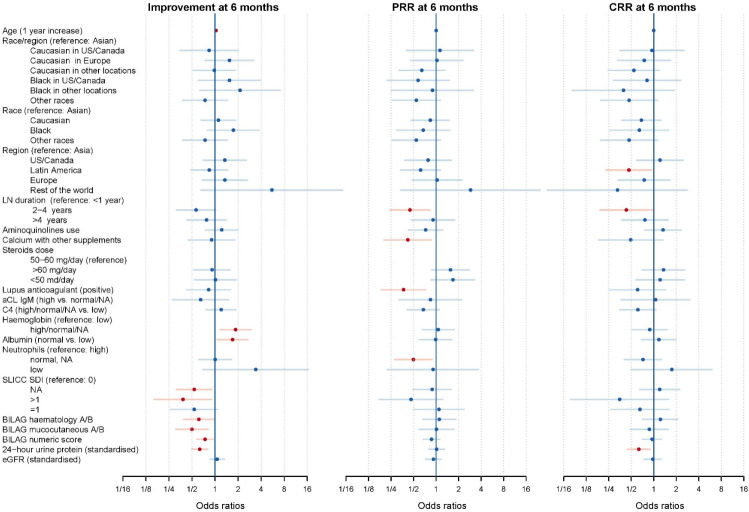
Results: We studied 370 patients in the ALMS induction trial. Improvement at 6 months was associated with older age (OR=1.03 (95% CI: 1.01 to 1.05) per year), normal haemoglobin (1.85 (1.16 to 2.95) vs low haemoglobin), active lupus (British Isles Lupus Assessment Group A or B) in haematological and mucocutaneous domains (0.61 (0.39 to 0.97) and 0.50 (0.31 to 0.81)), baseline damage (SDI>1 vs =0) (0.38 (0.16 to 0.91)) and 24-hour urine protein (0.63 (0.50 to 0.80)). LN duration 2-4 years (0.43 (0.19 to 0.97) vs <1 year) and 24-hour urine protein (0.63 (0.45 to 0.89)) were negative predictors of CRR. LN duration 2-4 years (0.45 (0.24 to 0.83) vs <1 year) negatively predicted PRR. The AUROCs of models for improvement, CRR and PRR were 0.56, 0.55 and 0.51 respectively.
Conclusions: Baseline variables predicted 6-month outcomes in patients with SLE. While the modest performance of models emphasises the need for new biomarkers to advance this field, the factors identified can help identify those patients who may require novel treatment strategies.
Keywords: cyclophosphamide; lupus nephritis; treatment.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: CG has received personal fees for honoraria from consultancy work and/or advisory boards from the Center for Disease Control, AstraZeneca, BMS, GSK, MGP, Sanofi, UCB, Aspreva Pharmaceuticals, Genentech and Roche Pharmaceuticals; personal fees for speakers bureau from UCB and GSK; previous educational grants from Aspreva Pharmaceuticals to the University of Birmingham, and from UCB to Sandwell and West Birmingham Hospitals NHS Trust that have supported her research work independent of any specific drug. LL and NS are employees of Aurinia Pharmaceuticals Inc. and holds stock in the company. LL and NS were both previously an employee of Aspreva Pharmaceuticals and Vifor Pharmaceuticals at the time of the conduct of the ALMS trial and held stock options in the companies. MT has a paid consultancy for Aurinia Pharmaceuticals Inc and previously held a paid consultancy for Aspreva Pharmaceuticals and Vifor Pharmaceuticals. INB has received grant/research support from Genzyme/Sanofi, GSK, Roche and UCB; received consulting fees from Eli Lilly, GSK, Merck Serono, UCB and ILTOO; and was a speaker for AstraZeneca, GSK and UCB.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical