

Ventilatory Ratio Is a Valuable Prognostic Indicator in an Observational Cohort of Patients With ARDS
- PMID: 35641002
- PMCID: PMC9994339
- DOI: 10.4187/respcare.09854
Ventilatory Ratio Is a Valuable Prognostic Indicator in an Observational Cohort of Patients With ARDS
Abstract
Background: How indices specific to respiratory compromise contribute to prognostication in patients with ARDS is not well characterized in general clinical populations. The primary objective of this study was to identify variables specific to respiratory failure that might add prognostic value to indicators of systemic illness severity in an observational cohort of subjects with ARDS.
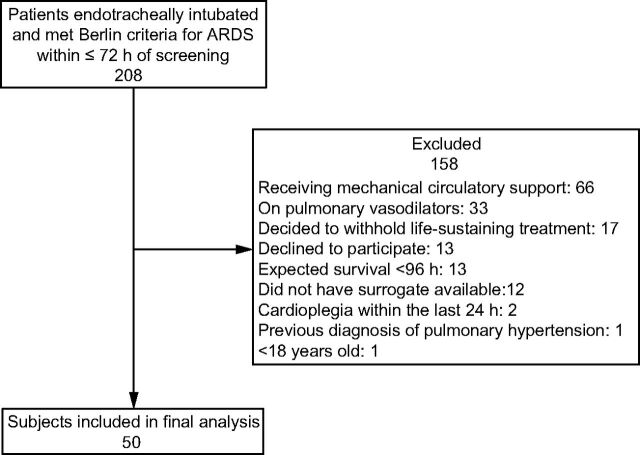
Methods: Fifty subjects with ARDS were enrolled in a single-center, prospective, observational cohort. We tested the contribution of respiratory variables (oxygenation index, ventilatory ratio [VR], and the radiographic assessment of lung edema score) to logistic regression models of 28-d mortality adjusted for indicators of systemic illness severity (the Acute Physiology and Chronic Health Evaluation [APACHE] III score or severity of shock as measured by the number of vasopressors required at baseline) using likelihood ratio testing. We also compared a model utilizing APACHE III with one including baseline number of vasopressors by comparing the area under the receiver operating curve (AUROC).
Results: VR significantly improved model performance by likelihood ratio testing when added to APACHE III (P = .036) or the number of vasopressors at baseline (P = .01). Number of vasopressors required at baseline had similar prognostic discrimination to the APACHE III. A model including the number of vasopressors and VR (AUROC 0.77 [95% CI 0.64-0.90]) was comparable to a model including APACHE III and VR (AUROC 0.81 [95% CI 0.68-0.93]; P for comparison = .58.).
Conclusions: In this observational cohort of subjects with ARDS, the VR significantly improved discrimination for mortality when combined with indicators of severe systemic illness. The number of vasopressors required at baseline and APACHE III had similar discrimination for mortality when combined with VR. VR is easily obtained at the bedside and offers promise for clinical prognostication.
Keywords: ARDS; pulmonary dead space; pulmonary edema; ventilatory ratio.
Copyright © 2022 by Daedalus Enterprises.
Conflict of interest statement
Dr Wick has received grant support from NIH, No. 5T32GM008440-24. The remaining authors have disclosed no conflicts of interest.
Figures
References
-
- Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest 1991;100(6):1619-1636. - PubMed
-
- Pais FM, Sinha P, Liu KD, Matthay MA. Influence of clinical factors and exclusion criteria on mortality in ARDS observational studies and randomized controlled trials. Respir Care 2018;63(8):1060-1069. - PubMed
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. ; ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin definition. JAMA 2012;307(23):2526-2533. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
