

Right ventricular function across the spectrum of health and disease
- PMID: 35641176
- PMCID: PMC9985748
- DOI: 10.1136/heartjnl-2021-320526
Right ventricular function across the spectrum of health and disease
Abstract
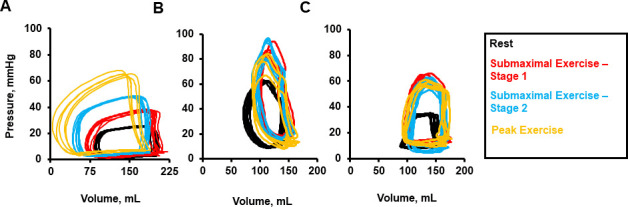
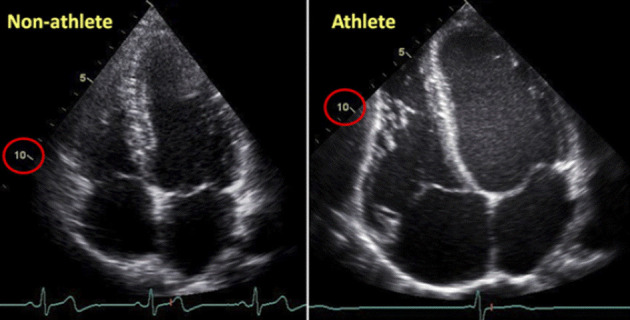
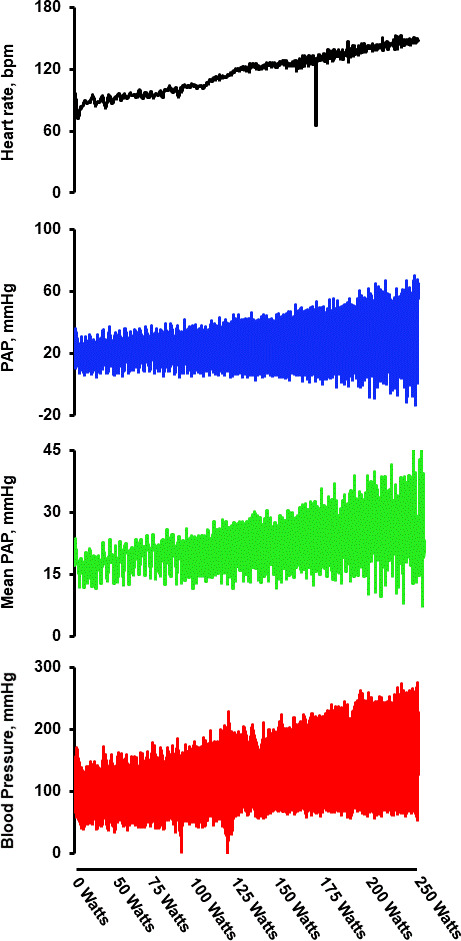
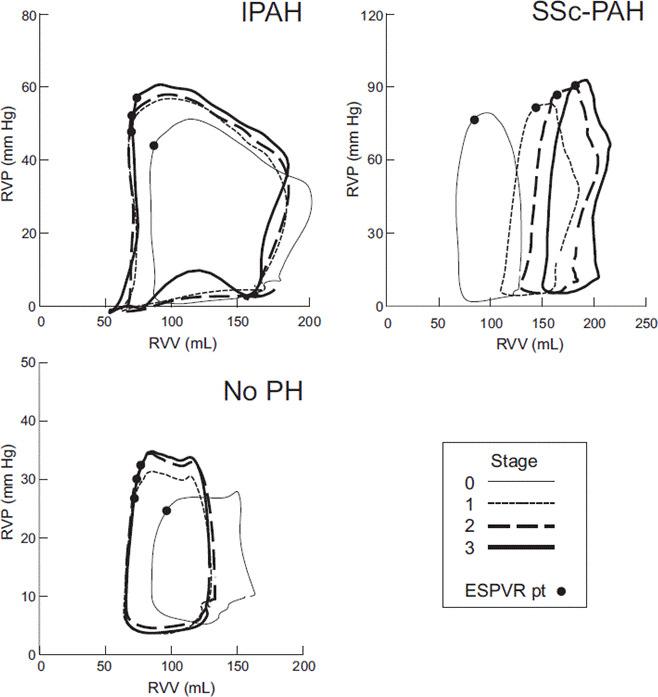
Knowledge of right ventricular (RV) structure and function has historically lagged behind that of the left ventricle (LV). However, advancements in invasive and non-invasive evaluations, combined with epidemiological analyses, have advanced the current understanding of RV (patho)physiology across the spectrum of health and disease, and reinforce the centrality of the RV in contributing to clinical outcomes. In the healthy heart, ventricular-arterial coupling is preserved during rest and in response to increased myocardial demand (eg, exercise) due to substantial RV contractile reserve. However, prolonged exposure to increased myocardial demand, such as endurance exercise, may precipitate RV dysfunction, suggesting that unlike the LV, the RV is unable to sustain high levels of contractility for extended periods of time. Emerging data increasingly indicate that both LV and RV function contribute to clinical heart failure. Reductions in quality-of-life, functional capacity and overall clinical outcomes are worsened among patients with heart failure when there is evidence of RV dysfunction. In addition, the RV is adversely impacted by pulmonary vascular disease, and among affected patients, overall RV function differs based on mechanisms of the underlying pulmonary hypertension, which may result from variations in sarcomere function within RV cardiomyocytes.
Keywords: Heart Failure; Pulmonary Arterial Hypertension.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
Pulmonary vascular mechanical consequences of ischemic heart failure and implications for right ventricular function.Am J Physiol Heart Circ Physiol. 2019 May 1;316(5):H1167-H1177. doi: 10.1152/ajpheart.00319.2018. Epub 2019 Feb 15. Am J Physiol Heart Circ Physiol. 2019. PMID: 30767670 Free PMC article.
-
The Right Heart-Pulmonary Circulation Unit in Systemic Hypertension.Heart Fail Clin. 2018 Jul;14(3):247-253. doi: 10.1016/j.hfc.2018.02.002. Heart Fail Clin. 2018. PMID: 29966624 Review.
-
Enhanced pulmonary vasodilator reserve and abnormal right ventricular: pulmonary artery coupling in heart failure with preserved ejection fraction.Circ Heart Fail. 2015 May;8(3):542-50. doi: 10.1161/CIRCHEARTFAILURE.114.002114. Epub 2015 Apr 9. Circ Heart Fail. 2015. PMID: 25857307 Clinical Trial.
-
Exercise right ventricular ejection fraction predicts right ventricular contractile reserve.J Heart Lung Transplant. 2021 Jun;40(6):504-512. doi: 10.1016/j.healun.2021.02.005. Epub 2021 Feb 17. J Heart Lung Transplant. 2021. PMID: 33752973 Free PMC article.
-
The Right Ventricle: From Embryologic Development to RV Failure.Curr Heart Fail Rep. 2022 Oct;19(5):325-333. doi: 10.1007/s11897-022-00572-z. Epub 2022 Sep 23. Curr Heart Fail Rep. 2022. PMID: 36149589 Free PMC article. Review.
Cited by
-
Mast Cells in Cardiac Remodeling: Focus on the Right Ventricle.J Cardiovasc Dev Dis. 2024 Feb 4;11(2):54. doi: 10.3390/jcdd11020054. J Cardiovasc Dev Dis. 2024. PMID: 38392268 Free PMC article. Review.
-
A pilot study on the hemodynamic effects of negative pressure ventilation in patients after cardiac surgery focussing on right ventricular function.Sci Rep. 2025 Jul 31;15(1):27974. doi: 10.1038/s41598-025-12534-1. Sci Rep. 2025. PMID: 40744972 Free PMC article.
-
Right Ventricular Function in Long-Term Survivors of Childhood Acute Lymphoblastic Leukemia: From the CTOXALL Study.Cancers (Basel). 2023 Oct 26;15(21):5158. doi: 10.3390/cancers15215158. Cancers (Basel). 2023. PMID: 37958333 Free PMC article.
-
Right ventricular performance during acute hypoxic exercise.J Physiol. 2024 Nov;602(21):5523-5537. doi: 10.1113/JP284943. Epub 2024 Feb 26. J Physiol. 2024. PMID: 38409819
-
Cardiac tissue engineering: an emerging approach to the treatment of heart failure.Front Bioeng Biotechnol. 2024 Aug 15;12:1441933. doi: 10.3389/fbioe.2024.1441933. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 39211011 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical