

Racial and Ethnic Disparities in Lung Cancer Screening by the 2021 USPSTF Guidelines Versus Risk-Based Criteria: The Multiethnic Cohort Study
- PMID: 35642317
- PMCID: PMC9156850
- DOI: 10.1093/jncics/pkac033
Racial and Ethnic Disparities in Lung Cancer Screening by the 2021 USPSTF Guidelines Versus Risk-Based Criteria: The Multiethnic Cohort Study
Abstract
Background: In 2021, the US Preventive Services Task Force (USPSTF) revised its lung cancer screening guidelines to expand screening eligibility. We evaluated screening sensitivities and racial and ethnic disparities under the 2021 USPSTF criteria vs alternative risk-based criteria in a racially and ethnically diverse population.
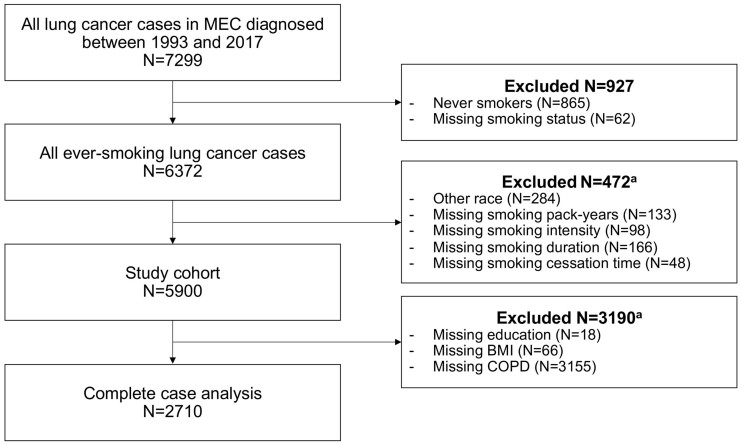
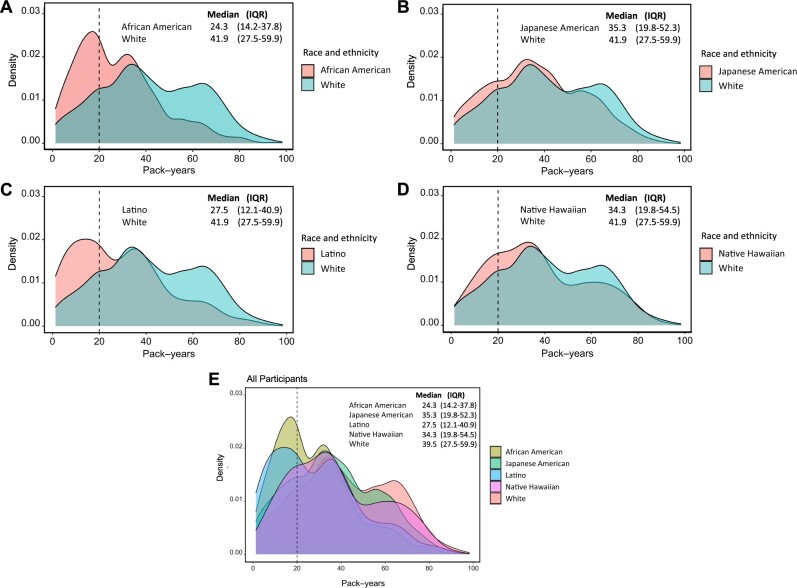
Methods: In the Multiethnic Cohort, we evaluated the proportion of ever-smoking lung cancer cases eligible for screening (ie, screening sensitivity) under the 2021 USPSTF criteria and under risk-based criteria through the PLCOm2012 model (6-year risk ≥1.51%). We also calculated the screening disparity (ie, absolute sensitivity difference) for each of 4 racial or ethnic groups (African American, Japanese American, Latino, Native Hawaiian) vs White cases.
Results: Among 5900 lung cancer cases, 43.3% were screen eligible under the 2021 USPSTF criteria. Screening sensitivities varied by race and ethnicity, with Native Hawaiian (56.7%) and White (49.6%) cases attaining the highest sensitivities and Latino (37.3%), African American (38.4%), and Japanese American (40.0%) cases attaining the lowest. Latino cases had the greatest screening disparity vs White cases at 12.4%, followed by African American (11.2%) and Japanese American (9.6%) cases. Under risk-based screening, the overall screening sensitivity increased to 75.7%, and all racial and ethnic groups had increased sensitivities (54.5%-91.9%). Whereas the screening disparity decreased to 5.1% for African American cases, it increased to 28.6% for Latino cases and 12.8% for Japanese American cases.
Conclusions: In the Multiethnic Cohort, racial and ethnic disparities decreased but persisted under the 2021 USPSTF lung cancer screening guidelines. Risk-based screening through PLCOm2012 may increase screening sensitivities and help to reduce disparities in some, but not all, racial and ethnic groups. Further optimization of risk-based screening strategies across diverse populations is needed.
© The Author(s) 2022. Published by Oxford University Press.
Figures
Comment in
-
A Feasible Path to Reductions in Racial and Ethnic Disparities in Lung Cancer Screening?JNCI Cancer Spectr. 2022 May 2;6(3):pkac034. doi: 10.1093/jncics/pkac034. JNCI Cancer Spectr. 2022. PMID: 35642318 Free PMC article. No abstract available.
References
-
- Becker N, Motsch E, Trotter A, et al.Lung cancer mortality reduction by LDCT screening-results from the randomized German LUSI trial. Int J Cancer. 2020;146(6):1503-1513. - PubMed
-
- de Koning HJ, van der Aalst CM, de Jong PA, et al.Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382(6):503-513. - PubMed
-
- Moyer VA; U.S. Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330-338. - PubMed
-
- US Preventive Services Task Force. Lung cancer: screening. 2020. https://www.uspreventiveservicestaskforce.org/uspstf/draft-update-summar.... Accessed December 2, 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical