

Managing Traumatic Brain Injury During the Coronavirus Disease 2019 Pandemic-A Case-Matched Controlled Analysis of Immediate Outcomes
- PMID: 35643408
- PMCID: PMC9131442
- DOI: 10.1016/j.wneu.2022.05.076
Managing Traumatic Brain Injury During the Coronavirus Disease 2019 Pandemic-A Case-Matched Controlled Analysis of Immediate Outcomes
Abstract
Objective: The primary objective of this study was to evaluate the outcome of patients with traumatic brain injury (TBI) during the coronavirus disease 2019 (COVID-19) pandemic and to compare their outcome with case-matched controls from the prepandemic phase.
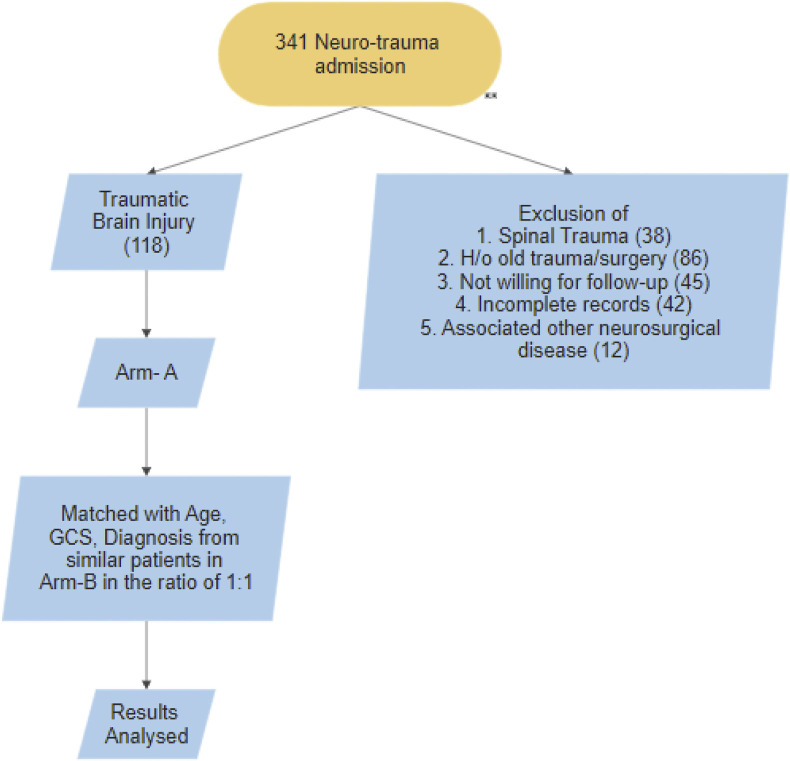
Methods: This is a retrospective case-control study in which all patients with TBI admitted during COVID-19 pandemic phase (Arm A) from March 24, 2020 to November 30, 2020 were matched with age and Glasgow Coma Scale score-matched controls from the patients admitted before March 2020 (Arm B).
Results: The total number of patients matched in each arm was 118. The length of hospital stay (8 days vs. 5 days; P < 0.001), transit time from emergency room to operation room (150 minutes vs. 97 minutes; P = 0.271), anesthesia induction time (75 minutes vs. 45 minutes; P = 0.002), and operative duration (275 minutes vs. 180 minutes; P = 0.002) were longer in arm A. Although the incidence of fever and pneumonia was significantly higher in arm A than in arm B (50% vs. 26.3%, P < 0.001 and 27.1% vs. 1.7%, P < 0.001, respectively), outcome (Glasgow Outcome Scale-Extended) and mortality (18.6% vs. 14.4% respectively; P = 0.42) were similar in both the groups.
Conclusions: The outcome of the patients managed for TBI during the COVID-19 pandemic was similar to matched patients with TBI managed at our center before the onset of the COVID-19 pandemic. This finding suggests that the guidelines followed during the COVID-19 pandemic were effective in dealing with patients with TBI. This model can serve as a guide for any future pandemic waves for effective management of patients with TBI without compromising their outcome.
Keywords: COVID-19; Outcome; Traumatic brain injury.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures





References
-
- Archived: WHO Timeline - COVID-19. https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 Available at:
-
- Raheja A., Sinha S., Samson N., et al. Serum biomarkers as predictors of long-term outcome in severe traumatic brain injury: analysis from a randomized placebo-controlled phase II clinical trial. J Neurosurg. 2016;125:631–641. - PubMed
-
- Raheja A., Agarwal N., Mohapatra S., et al. Preparedness and guidelines for neurosurgery in the COVID-19 era: Indian perspective from a tertiary care referral hospital. Neurosurg Focus. 2020;49:E3. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
