

Association of ambulatory blood pressure with coronary microvascular and cardiac dysfunction in asymptomatic type 2 diabetes
- PMID: 35643571
- PMCID: PMC9148453
- DOI: 10.1186/s12933-022-01528-2
Association of ambulatory blood pressure with coronary microvascular and cardiac dysfunction in asymptomatic type 2 diabetes
Abstract
Background: Type 2 diabetes (T2D) and hypertension commonly coexist and are associated with subclinical myocardial structural and functional changes. We sought to determine the association between blood pressure (BP) and left ventricular (LV) remodeling, systolic/diastolic function, and coronary microvascular function, among individuals with T2D without prevalent cardiovascular disease.
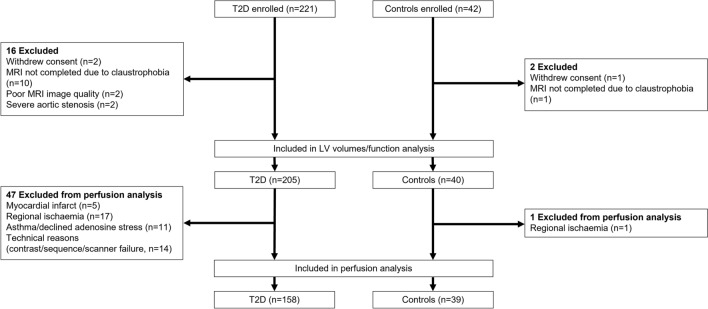
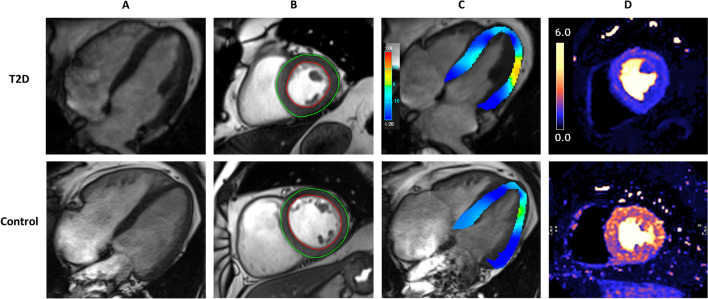
Methods: Participants with T2D and age-, sex-, and ethnicity-matched controls underwent comprehensive cardiovascular phenotyping including fasting bloods, transthoracic echocardiography, cardiovascular magnetic resonance imaging with quantitative adenosine stress/rest perfusion, and office and 24-h ambulatory BP monitoring. Multivariable linear regression was performed to determine independent associations between BP and imaging markers of remodeling and function in T2D.
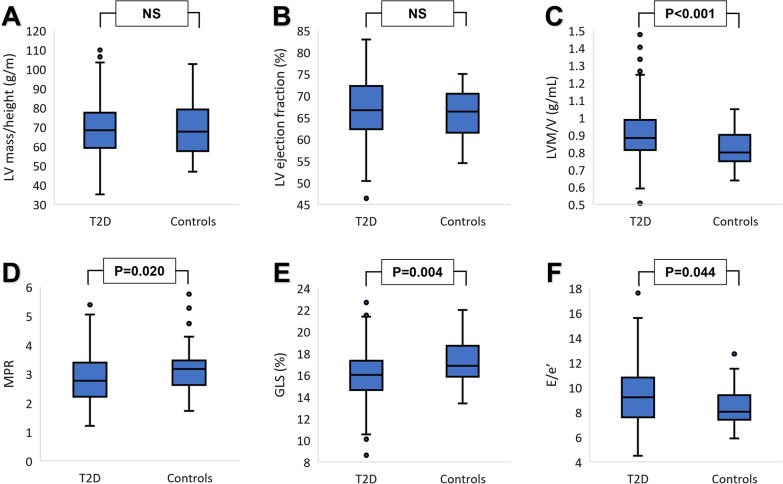
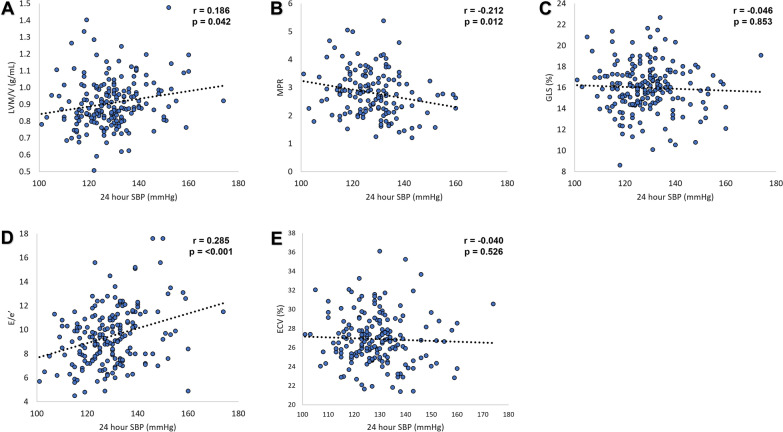
Results: Individuals with T2D (n = 205, mean age 63 ± 7 years) and controls (n = 40, mean age 61 ± 8 years) were recruited. Mean 24-h systolic BP, but not office BP, was significantly greater among those with T2D compared to controls (128.8 ± 11.7 vs 123.0 ± 13.1 mmHg, p = 0.006). Those with T2D had concentric LV remodeling (mass/volume 0.91 ± 0.15 vs 0.82 ± 0.11 g/mL, p < 0.001), decreased myocardial perfusion reserve (2.82 ± 0.83 vs 3.18 ± 0.82, p = 0.020), systolic dysfunction (global longitudinal strain 16.0 ± 2.3 vs 17.2 ± 2.1%, p = 0.004) and diastolic dysfunction (E/e' 9.30 ± 2.43 vs 8.47 ± 1.53, p = 0.044) compared to controls. In multivariable regression models adjusted for 14 clinical variables, mean 24-h systolic BP was independently associated with concentric LV remodeling (β = 0.165, p = 0.031), diastolic dysfunction (β = 0.273, p < 0.001) and myocardial perfusion reserve (β = - 0.218, p = 0.016). Mean 24-h diastolic BP was associated with LV concentric remodeling (β = 0.201, p = 0.016).
Conclusion: 24-h ambulatory systolic BP, but not office BP, is independently associated with cardiac remodeling, coronary microvascular dysfunction, and diastolic dysfunction among asymptomatic individuals with T2D. (Clinical trial registration. URL: https://clinicaltrials.gov/ct2/show/NCT03132129 Unique identifier: NCT03132129).
Keywords: Ambulatory blood pressure; Blood pressure; Diabetic cardiomyopathy; Myocardial perfusion reserve; Type 2 diabetes.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Colvin MM, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70(6):776–803. doi: 10.1016/j.jacc.2017.04.025. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- FS/16/47/32190/BHF_/British Heart Foundation/United Kingdom
- FS/CRTF/20/24069/BHF_/British Heart Foundation/United Kingdom
- FS/18/26/33501/BHF_/British Heart Foundation/United Kingdom
- RP-2017-08-ST2-007/DH_/Department of Health/United Kingdom
- FS/TF/21/33008/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
