

Update on the pathogenesis of vitiligo
- PMID: 35643735
- PMCID: PMC9263675
- DOI: 10.1016/j.abd.2021.09.008
Update on the pathogenesis of vitiligo
Abstract
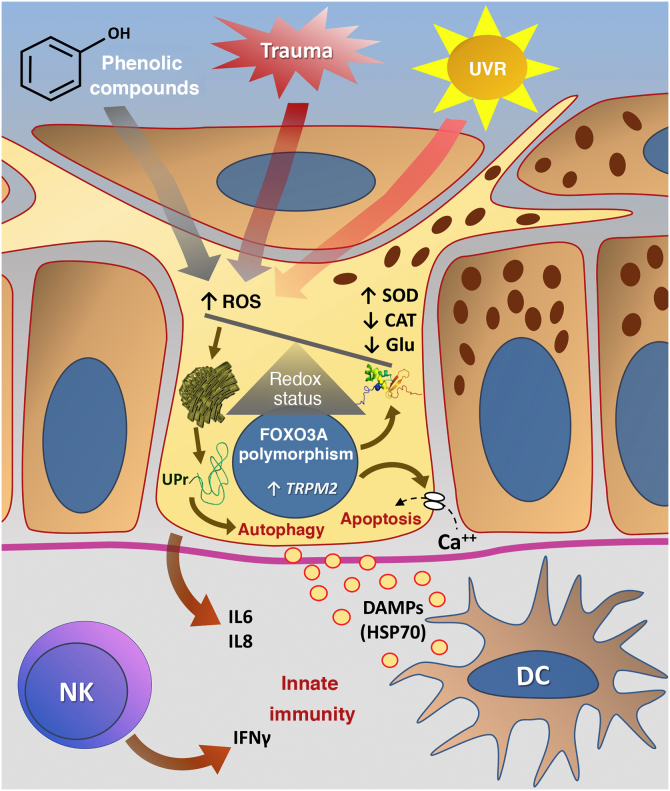
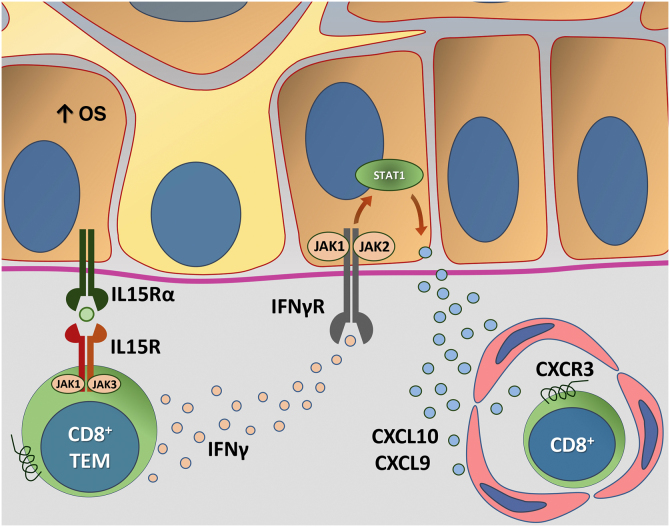
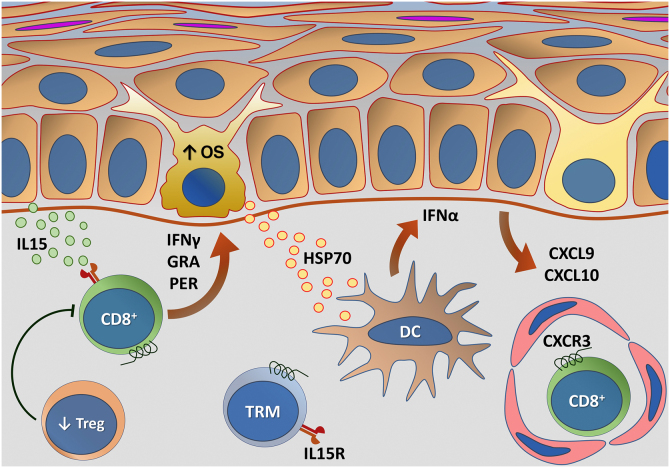
Vitiligo is a complex disease whose pathogenesis results from the interaction of genetic components, metabolic factors linked to cellular oxidative stress, melanocyte adhesion to the epithelium, and immunity (innate and adaptive), which culminate in aggression against melanocytes. In vitiligo, melanocytes are more sensitive to oxidative damage, leading to the increased expression of proinflammatory proteins such as HSP70. The lower expression of epithelial adhesion molecules, such as DDR1 and E-cadherin, facilitates damage to melanocytes and exposure of antigens that favor autoimmunity. Activation of the type 1-IFN pathway perpetuates the direct action of CD8+ cells against melanocytes, facilitated by regulatory T-cell dysfunction. The identification of several genes involved in these processes sets the stage for disease development and maintenance. However, the relationship of vitiligo with environmental factors, psychological stress, comorbidities, and the elements that define individual susceptibility to the disease are a challenge to the integration of theories related to its pathogenesis.
Keywords: Autoimmunity; Oxidative stress; Pigmentation; Vitiligo.
Copyright © 2022 Sociedade Brasileira de Dermatologia. Published by Elsevier España, S.L.U. All rights reserved.
Figures

References
-
- Castro CCS, Miot HA. Prevalence of vitiligo in Brazil—a population survey. Pigment Cell Melanoma Res. 2018;31:448–450. - PubMed
-
- Castro C.C.S., Nascimento L.L.M., Olandoski M., Mira M.T. A pattern of association between clinical form of vitiligo and disease-related variables in a Brazilian population. J Dermatol Sci. 2012;65:63–67. - PubMed
-
- Boza J.C., Giongo N., Machado P., Horn R., Fabbrin A., Cestari T. Quality of life impairment in children and adults with vitiligo: a cross-sectional study based on dermatology-specific and disease-specific quality of life instruments. Dermatology. 2016;232:619–625. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
