

Accuracy of MRI-CT registration in brain stereotactic radiotherapy: Impact of MRI acquisition setup and registration method
- PMID: 35643799
- PMCID: PMC9948832
- DOI: 10.1016/j.zemedi.2022.04.004
Accuracy of MRI-CT registration in brain stereotactic radiotherapy: Impact of MRI acquisition setup and registration method
Abstract
Background: In MR-based radiotherapy (RT), MRI images are co-registered to the planning CT to leverage MR image information for RT planning. Especially in brain stereotactic RT, where typical CTV-PTV margins are 1-2 mm, high registration accuracy is critical. Several factors influence the registration accuracy, including the acquisition setup during MR simulation and the registration methods.
Purpose: In this work, the impact of the MRI acquisition setup and registration method was evaluated in the context of brain RT, both geometrically and dosimetrically.
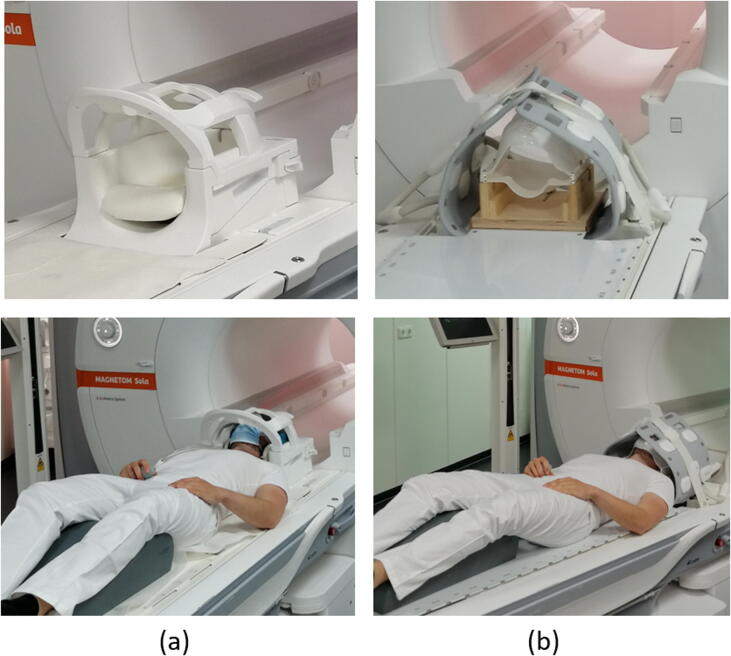
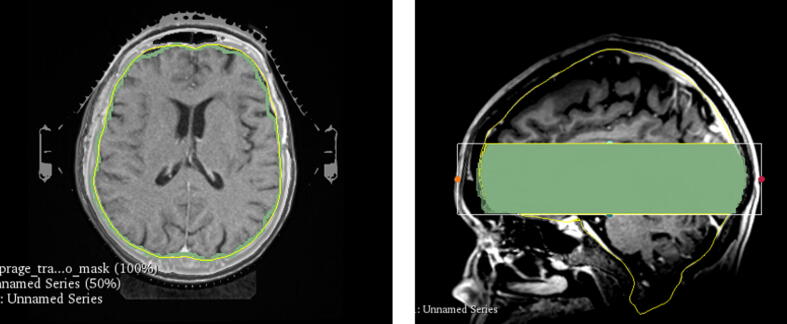
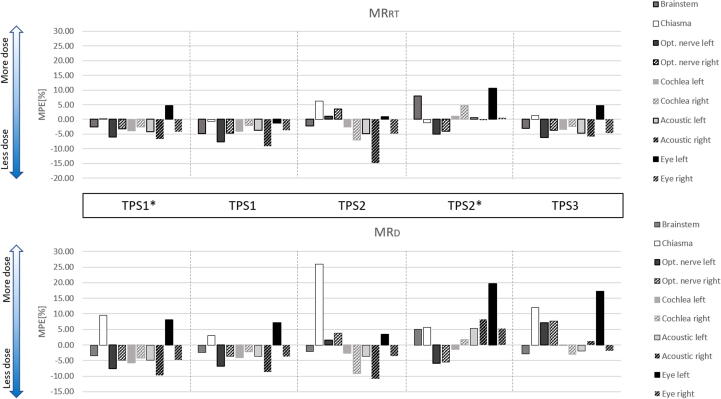
Methods and materials: MRI of 20 brain radiotherapy patients was acquired in two MRI acquisition setups (RT and diagnostic). Three different automatic registration tools provided by three treatment planning systems were used to rigidly register both MRIs and CT in addition to the clinical registration. Segmentation-based evaluation using Hausdorff Distance (HD)/Dice Similarity Coefficient and landmark-based evaluation were used as evaluation metrics. Dose-volume-histograms were evaluated for target volumes and various organs at risks.
Results: MRI acquisition in the RT setup provided a similar head extension as compared to the planning CT. The registration method had a more significant influence than the acquisition setup (Wilcoxon signed-rank test, p<0.05). When registering using a less optimal registration method, the RT setup improved the registration accuracy compared to the diagnostic setup (Difference: ΔMHD = 0.16 mm, ΔHDP95 = 0.64 mm, mean Euclidean distance (ΔmEuD) = 2.65 mm). Different registration methods and acquisition setups lead to the variation of the clinical DVH. Acquiring MRI in the RT setup can improve PTV and GTV coverage compared to the diagnostic setup.
Conclusions: Both MRI acquisition setup and registration method influence the MRI-CT registration accuracy in brain RT patients geometrically and dosimetrically. MR-simulation in the RT setup assures optimal registration accuracy if automatic registration is impaired, and therefore recommended for brain RT.
Keywords: Brain radiotherapy; Intracranial stereotactic radiotherapy; Magnetic-resonance imaging; Patient immobilization; Registration.
Copyright © 2022. Published by Elsevier GmbH.
Conflict of interest statement
Declaration of Competing Interest Universitätsklinikum Erlangen, Strahlenklinik and Siemens Healthineers (Erlangen, Germany) have institutional research contracts not related to this specific work. Christoph Bert and Florian Putz act as speakers in training courses of Siemens Healthineers.
Figures





References
-
- Kocher M., et al. Stereotactic radiosurgery for treatment of brain metastases. A report of the DEGRO Working Group on Stereotactic Radiotherapy. Strahlenther Onkol. 2014;190(6):521–532. - PubMed
-
- Schell M.C., No R., et al. 054 -Stereotactic Radiosurgery. Am Assoc Phys Med. 1995
-
- Salkeld A.L., et al. Changes in brain metastasis during radiosurgical planning. Int J Radiat Oncol Biol Phys. 2018;102(4):727–733. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
