

Dynamics of circulating calprotectin accurately predict the outcome of moderate COVID-19 patients
- PMID: 35644124
- PMCID: PMC9132728
- DOI: 10.1016/j.ebiom.2022.104077
Dynamics of circulating calprotectin accurately predict the outcome of moderate COVID-19 patients
Abstract
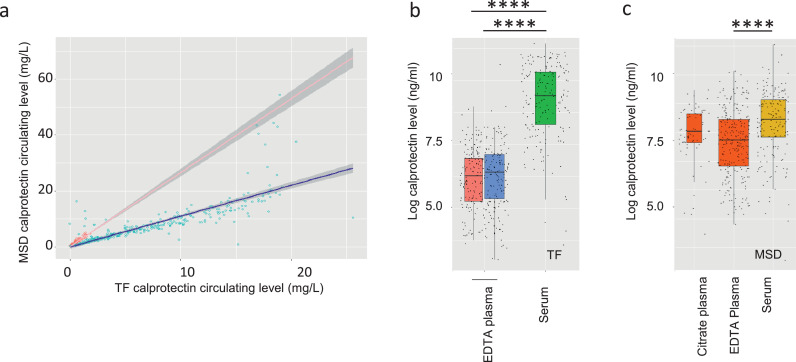
Background: Severe COVID-19 is associated with a high circulating level of calprotectin, the S100A8/S100A9 alarmin heterodimer. Baseline calprotectin amount measured in peripheral blood at diagnosis correlates with disease severity. The optimal use of this biomarker along COVID-19 course remains to be delineated.
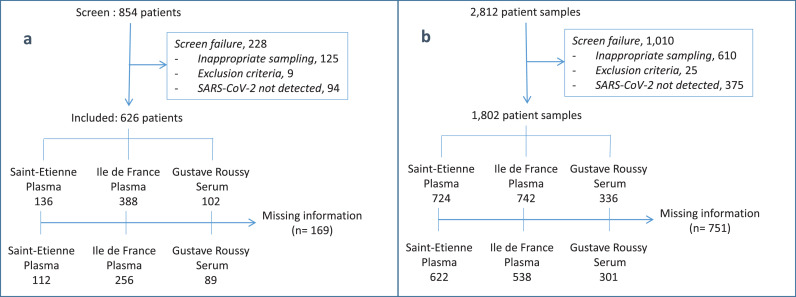
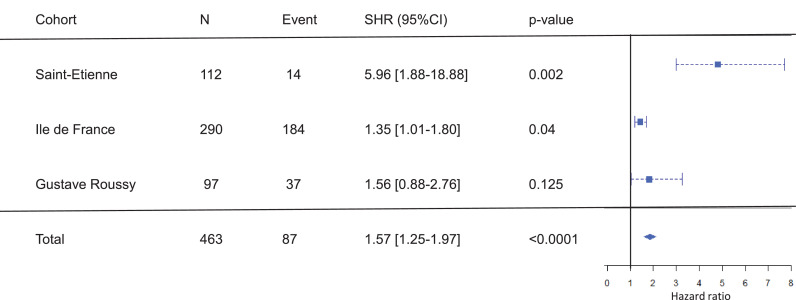
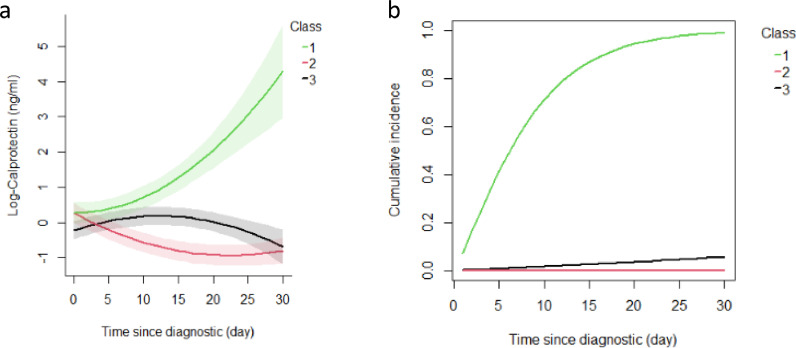
Methods: We focused on patients with a WHO-defined moderate COVID-19 requiring hospitalization in a medical ward. We collected plasma and serum from three independent cohorts (N = 626 patients) and measured calprotectin amount at admission. We performed longitudinal measures of calprotectin in 457 of these patients (1461 samples) and used a joint latent class mixture model in which classes were defined by age, body mass index and comorbidities to identify calprotectin trajectories predicting the risk of transfer into an intensive care unit or death.
Findings: After adjustment for age, sex, body mass index and comorbidities, the predictive value of baseline calprotectin in patients with moderate COVID19 could be refined by serial monitoring of the biomarker. We discriminated three calprotectin trajectories associated with low, moderate, and high risk of poor outcome, and we designed an algorithm available as online software (https://calpla.gustaveroussy.fr:8443/) to monitor the probability of a poor outcome in individual patients with moderate COVID-19.
Interpretation: These results emphasize the clinical interest of serial monitoring of calprotectin amount in the peripheral blood to anticipate the risk of poor outcomes in patients with moderate COVID-19 hospitalized in a standard care unit.
Funding: The study received support (research grants) from ThermoFisher immunodiagnostics (France) and Gustave Roussy Foundation.
Keywords: Biomarker; COVID-19; Calprotectin; Dynamics; S100A8/A9; Serial measurement.
Copyright © 2022 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
This study (NI, TB, CG, AEB, MA, CCG, AB, LC, RC, BD, JD, MD, FF, AP, FP, OS, DMS, TAS, AS, LL, GJC, SR, BP, DD, MF, SH, SP, ES) received support of a research grant provided by ThermoFisher Immunodiagnostics; CM and LS are employees of Thermo Fisher Scientific; FA received institutional grants from Roche, Astra Zeneca, Daichy Sankyo, Pfizer, Novartis, and Lilly; NG received consultation fees from Bayer, Leo Pharma, Aspen, Sanofi and honoraria from Boehringer Ingelheim, Bristol Myers Squib, Pfizer, and Leo Pharma; TM received honoraria and supports for attending meetings from BAYER HealthCare and Incyte Biosciences France; FP received a grant from Alexion, consulting fees and honoraria from Gilead.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
