

Outcomes and Predictors of 28-Day Mortality in Patients With Solid Tumors and Septic Shock Defined by Third International Consensus Definitions for Sepsis and Septic Shock Criteria
- PMID: 35644244
- PMCID: PMC9808606
- DOI: 10.1016/j.chest.2022.05.017
Outcomes and Predictors of 28-Day Mortality in Patients With Solid Tumors and Septic Shock Defined by Third International Consensus Definitions for Sepsis and Septic Shock Criteria
Abstract
Background: Data assessing outcomes of patients with solid tumors demonstrating septic shock using the Third International Consensus Definitions for Sepsis and Septic Shock are scarce.
Research question: What are the independent predictors of 28-day mortality in critically ill adults with solid tumors and septic shock?
Study design and methods: Cohort of solid tumor patients admitted to the ICU with septic shock. Demographic and clinical characteristics were gathered from the electronic health records. We developed a reduced multivariate logistics regression model to identify independent predictors of 28-day mortality and used Kaplan-Meier plots to assess survival.
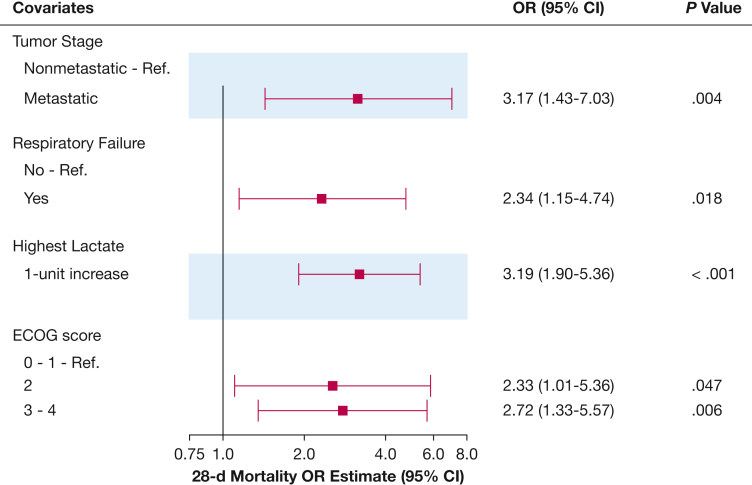
Results: A total of 271 patients were included. The median age was 62 years (range, 19-94 years); 57.2% were men and 53.5% were White. The most common underlying malignancies were lung (19.2%), breast (7.7%), pancreatic (7.7%), and colorectal (7.4%) cancers. Most patients (84.5%) harbored metastatic disease. Twenty-eight days after ICU admission, 188 patients (69.4%) had died. Nonsurvivors showed a higher rate of advanced cancer, longer hospital stays before ICU admission, and higher Sequential Organ Failure Assessment scores at admission and throughout the ICU stay (P < .001 for all). The multivariate analysis identified metastatic disease (OR, 3.17; 95% CI, 1.43-7.03), respiratory failure (OR, 2.34; 95% CI, 1.15-4.74), elevated lactate levels (OR, 3.19; 95% CI, 1.90-5.36), and Eastern Cooperative Oncology Group performance scores of 3 or 4 (OR, 2.72; 95% CI, 1.33-5.57) as independent predictors of 28-day mortality. Only 38 patients (14%) were discharged home without medical assistance.
Interpretation: The 28-day mortality rate of patients with solid tumors and septic shock was considerably high. Factors associated with worse survival included advanced oncologic disease, poor performance status, high lactate level, and concomitant acute respiratory failure. Early goals-of-care discussions should be considered for frail patients with septic shock and advanced metastatic disease without denying access to the appropriate level of care.
Keywords: ICU; cancer; complications; critical care; mortality; sepsis; septic shock; solid tumors.
Copyright © 2022 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures



Comment in
-
Septic Shock in Patients With Solid Malignancies: What Does the Host Response Yield When the Host Is Already Under Threat?Chest. 2022 Nov;162(5):951-953. doi: 10.1016/j.chest.2022.06.035. Chest. 2022. PMID: 36344119 No abstract available.
References
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. - PubMed
-
- Vento S., Cainelli F., Temesgen Z. Lung infections after cancer chemotherapy. Lancet Oncol. 2008;9(10):982–992. - PubMed
-
- Azoulay E., Mokart D., Pène F., et al. Outcomes of critically ill patients with hematologic malignancies: prospective multicenter data from France and Belgium—a groupe de recherche respiratoire en réanimation onco-hématologique study. J Clin Oncol. 2013;31(22):2810–2818. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
