

Placental Pathology After SARS-CoV-2 Infection in the Pre-Variant of Concern, Alpha / Gamma, Delta, or Omicron Eras
- PMID: 35645148
- PMCID: PMC9152633
- DOI: 10.1177/10668969221102534
Placental Pathology After SARS-CoV-2 Infection in the Pre-Variant of Concern, Alpha / Gamma, Delta, or Omicron Eras
Abstract
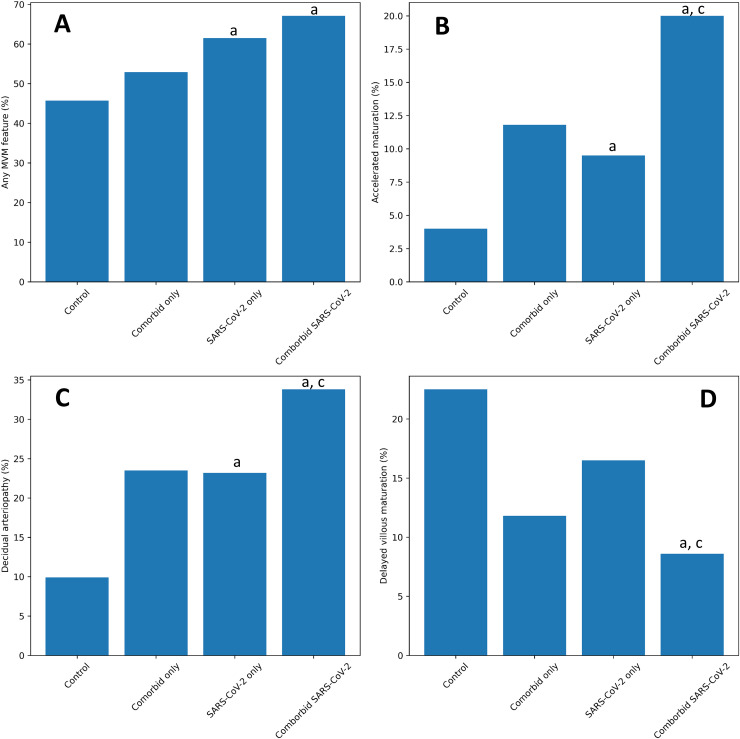
Objectives. The goal of this study is to describe placental pathology after infection with SARS-CoV-2 before the predominance of variants of concern (pre-VOC) and during eras of predominant transmission of the Alpha & Gamma (co-circulating), Delta, and Omicron variants. Methods. We used county-level variant data to establish population-level variant proportions, SARS-CoV-2 PCR to identify cases, and IgG serology to exclude latent infections from controls and histopathologic examination to identify placental pathology. Results. We report findings in 870 placentas from pregnancies complicated by SARS-CoV-2 including 90 with infection in the Alpha/Gamma era, 60 from the Delta era and 56 from the Omicron era. Features of maternal vascular malperfusion (MVM), including decidual arteriopathy, were significantly more frequent after SARS-CoV-2 infection. The risk of these findings varied over time, with the highest rates in the Delta era. Increased COVID-19 severity and the presence of comorbidities strengthened these associations. Conclusion. MVM is a feature of SARS-CoV-2 infection in pregnancy. Lesion frequency changed with the predominant circulating virus and should be considered with new variants.
Keywords: COVID-19; SARS-CoV-2; decidual arteriopathy; maternal vascular malperfusion; placenta; variants of concern.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures





References
-
- Zambrano LD. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy Status — United States, January 22–October 3, 2020. MMWR Morb Mortal Wkly Rep 2020;69. Available at: https://www.cdc.gov/mmwr/volumes/69/wr/mm6944e3.htm. Accessed November 30, 2021. - PMC - PubMed
-
- Karasek D, Baer RJ, McLemore MR, et al. The association of COVID-19 infection in pregnancy with preterm birth: a retrospective cohort study in California. Lancet Reg Health – Am 2021;2. Available at:https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(21)00019-.... Accessed November 30, 2021. - PMC - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
