

Bacterial and Fungal Co-Infections and Superinfections in a Cohort of COVID-19 Patients: Real-Life Data from an Italian Third Level Hospital
- PMID: 35645220
- PMCID: PMC9149992
- DOI: 10.3390/idr14030041
Bacterial and Fungal Co-Infections and Superinfections in a Cohort of COVID-19 Patients: Real-Life Data from an Italian Third Level Hospital
Abstract
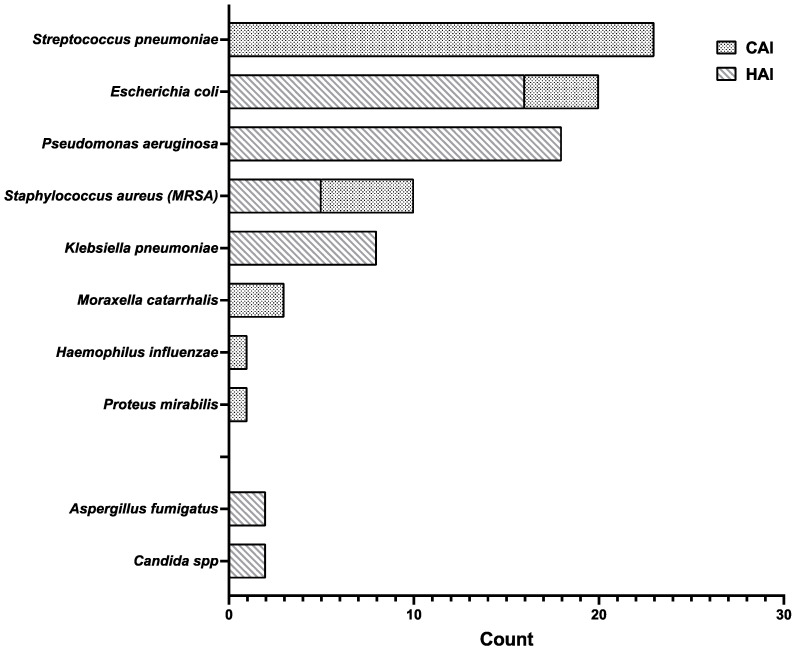
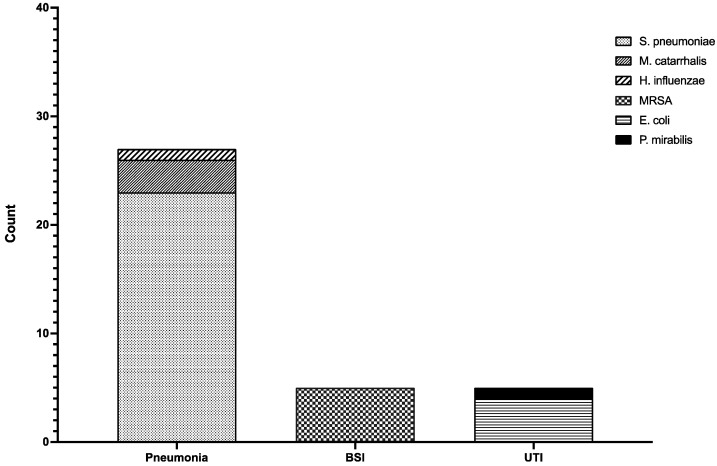
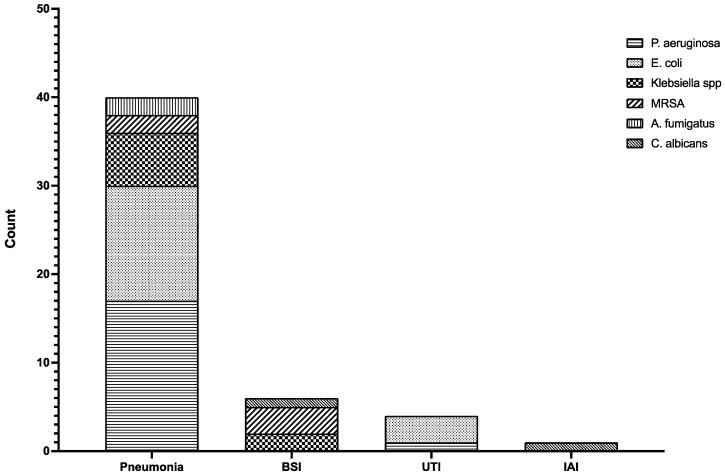
The use of immune suppressive drugs combined with the natural immune suppression caused by SARS-CoV-2 can lead to a surge of secondary bacterial and fungal infections. The aim of this study was to estimate the incidence of superinfections in hospitalized subjects with COVID-19. We carried out an observational retrospective single center cohort study. We enrolled patients admitted at the "Garibaldi" hospital for ≥72 h, with a confirmed diagnosis of COVID-19. All patients were routinely investigated for bacterial, viral, and fungal pathogens. A total of 589 adults with COVID-19 were included. A total of 88 infections were documented in different sites among 74 patients (12.6%). As for the etiology, 84 isolates were bacterial (95.5%), while only 4 were fungal (4.5%). A total of 51 episodes of hospital-acquired infections (HAI) were found in 43 patients, with a bacterial etiology in 47 cases (92.2%). Community-acquired infections (CAIs) are more frequently caused by Streptococcus pneumoniae, while HAIs are mostly associated with Pseudomonas aeruginosa. A high rate of CAIs and HAIs due to the use of high-dose corticosteroids and long hospital stays can be suspected. COVID-19 patients should be routinely evaluated for infection and colonization. More data about antimicrobial resistance and its correlation with antibiotic misuse in COVID-19 patients are required.
Keywords: COVID-19; bacterial; coinfections; community-acquired infection (CAI); fungal; hospital-acquired infection (HAI); superinfections.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ceccarelli M., Rullo E.V., Marino A., Cacopardo B., Berretta M., Nunnari G. Remdesivir Effectiveness in COVID-19 and Recommendations for Its Use. Infect. Dis. Trop. Med. 2020;6:e596. doi: 10.32113/idtm_20203_596. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
