

The ratio of superior mesenteric artery diameter to superior mesenteric vein diameter based on non-enhanced computed tomography in the early diagnosis of spontaneous isolated superior mesenteric artery dissection
- PMID: 35646218
- PMCID: PMC9108917
- DOI: 10.5847/wjem.j.1920-8642.2022.045
The ratio of superior mesenteric artery diameter to superior mesenteric vein diameter based on non-enhanced computed tomography in the early diagnosis of spontaneous isolated superior mesenteric artery dissection
Abstract
Background: Spontaneous isolated superior mesenteric artery (SMA) dissection (SISMAD) is a rare cause of abdominal pain. The aim of the study is to investigate the role of a new parameter, the ratio of the SMA diameter to the superior mesenteric vein (SMV) diameter (SMA/SMV) based on non-enhanced computed tomography (CT), in the early diagnosis of SISMAD.
Methods: In a registry study from December 2013 to June 2021, 97 abdominal pain SISMAD patients (SISMAD group) admitted to our hospital were enrolled. Meanwhile, the matched sex and age abdominal pain non-SISMAD patients at 1:2 were collected in reverse chronological order as the control group. Student's t-test, Wilcoxon rank-sum test, and Chi-square test were used to compare differences between the SISMAD and control groups. MedCalc was used to generate receiver operating characteristic (ROC) curve.
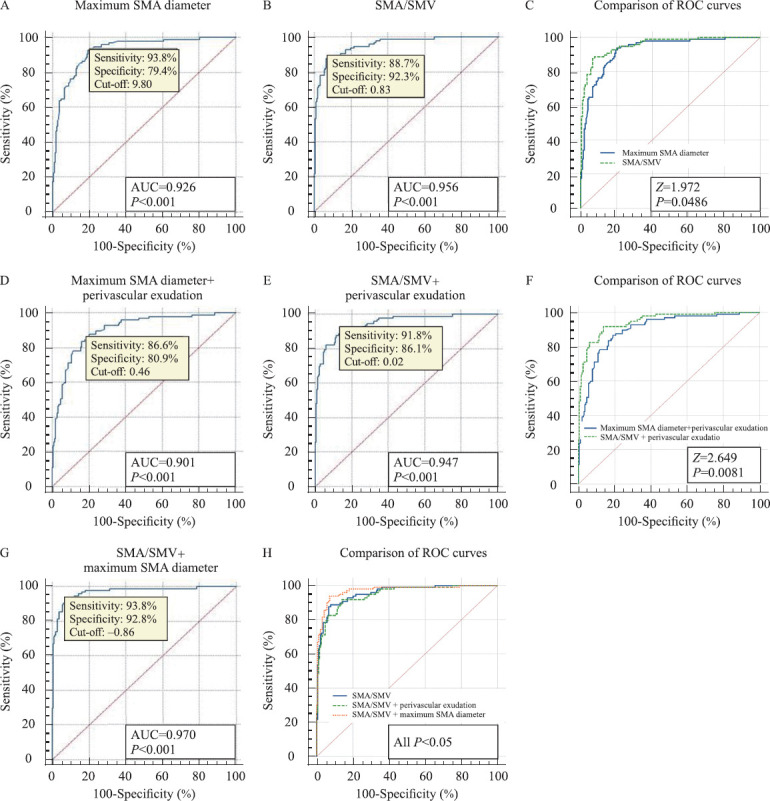
Results: A total of 291 abdominal pain patients, including 97 SISMAD patients and 194 non-SISMAD patients, were included in the current study. The maximum SMA diameter, perivascular exudation, and SMA/SMV based on non-enhanced CT were significant between the two groups (all P<0.05). ROC curves showed that for the maximum SMA diameter, the area under the curve (AUC), cut-off, sensitivity, and specificity were 0.926, 9.80, 93.8%, and 79.4%, respectively. For SMA/SMV, its AUC, cut-off, sensitivity, and specificity were 0.956, 0.83, 88.7%, and 92.3%, respectively. The diagnostic efficiency of SMA/SMV was better than that of the maximum SMA diameter (P<0.05). The combined parameters of SMA/SMV and maximum SMA diameter had the best diagnostic efficiency (AUC=0.970).
Conclusion: SMA/SMV may be a potential marker for SISMAD.
Keywords: Abdominal pain; Computed tomography; Receiver operating characteristic curve; Spontaneous isolated superior mesenteric artery dissection.
Copyright: © World Journal of Emergency Medicine.
Conflict of interest statement
Conflicts of interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Clinical characteristics and misdiagnosis of spontaneous isolated superior mesenteric artery dissection.BMC Cardiovasc Disord. 2022 May 25;22(1):239. doi: 10.1186/s12872-022-02676-9. BMC Cardiovasc Disord. 2022. PMID: 35610570 Free PMC article.
-
Clinical implications of perivascular fat stranding surrounding spontaneous isolated superior mesenteric artery dissection on computed tomography.Exp Ther Med. 2021 Jan;21(1):34. doi: 10.3892/etm.2020.9466. Epub 2020 Nov 11. Exp Ther Med. 2021. PMID: 33262820 Free PMC article.
-
The Significance of the Angle between Superior Mesenteric Artery and Aorta in Spontaneous Isolated Superior Mesenteric Artery Dissection.Ann Vasc Surg. 2017 Nov;45:117-126. doi: 10.1016/j.avsg.2017.06.156. Epub 2017 Jul 8. Ann Vasc Surg. 2017. PMID: 28689953
-
Systematic review and meta-analysis of current evidences in endograft therapy vs. medical treatment for Spontaneous Isolated Superior Mesenteric Artery Dissection.Langenbecks Arch Surg. 2024 Jul 15;409(1):215. doi: 10.1007/s00423-024-03406-9. Langenbecks Arch Surg. 2024. PMID: 39008150
-
Current Understandings of Spontaneous Isolated Superior Mesenteric Artery Dissection.Vasc Specialist Int. 2016 Jun;32(2):37-43. doi: 10.5758/vsi.2016.32.2.37. Epub 2016 Jun 30. Vasc Specialist Int. 2016. PMID: 27386450 Free PMC article. Review.
References
-
- Mkangala AM, Liang HM, Dong XJ, Su YB, Lu HH. Safety and efficacy of conservative, endovascular bare stent and endovascular coil assisting bare stent treatments for patients diagnosed with spontaneous isolated superior mesenteric artery dissection. Wideochir Inne Tech Maloinwazyjne. 2020;15(4):608–19. - PMC - PubMed
-
- Shi YD, Ni GQ, Zhao BX, Gu JP, Huang H, Lu ZX, et al. Management of symptomatic spontaneous isolated superior mesenteric artery dissection:a single centre experience with mid term follow up. Eur J Vasc Endovasc Surg. 2020;60(6):863–71. - PubMed
-
- Qiu CY, He YY, Li DL, Shang T, Wang XH, Wu ZH, et al. Mid-term results of endovascular treatment for spontaneous isolated dissection of the superior mesenteric artery. Eur J Vasc Endovasc Surg. 2019;58(1):88–95. - PubMed
LinkOut - more resources
Full Text Sources