

Arthroscopic Resection of Symptomatic Tibial Tubercle Ossicles for Recalcitrant Osgood-Schlatter Disease Using a 2-Portal Technique
- PMID: 35646564
- PMCID: PMC9134260
- DOI: 10.1016/j.eats.2021.12.041
Arthroscopic Resection of Symptomatic Tibial Tubercle Ossicles for Recalcitrant Osgood-Schlatter Disease Using a 2-Portal Technique
Abstract
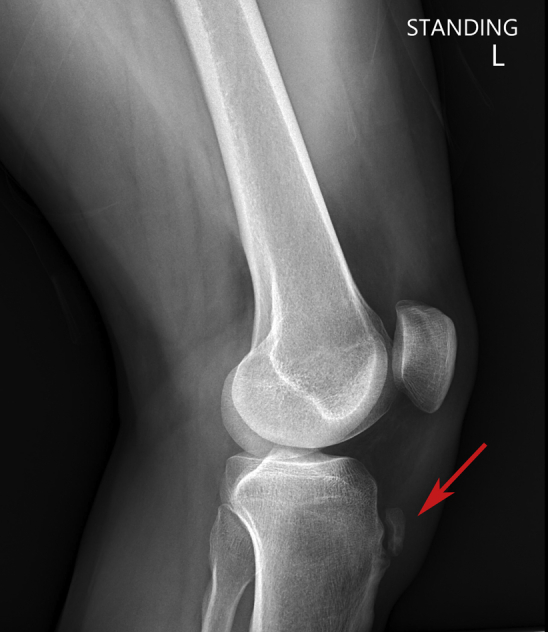
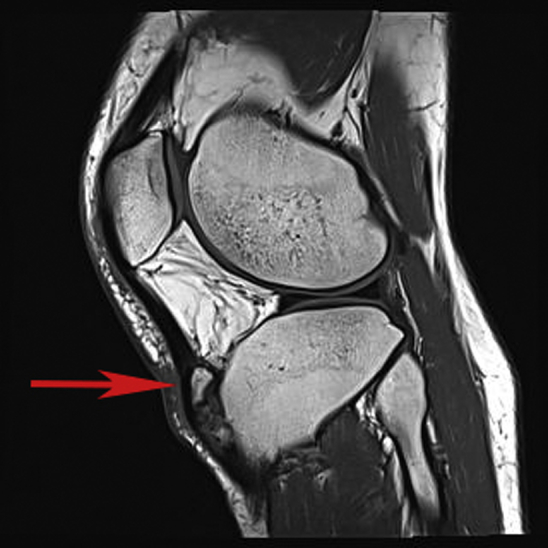
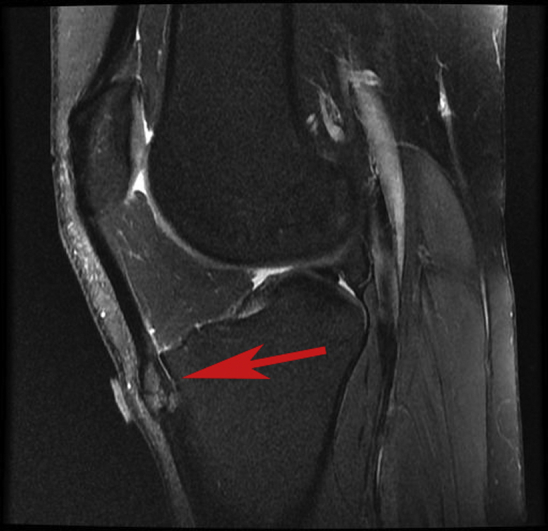
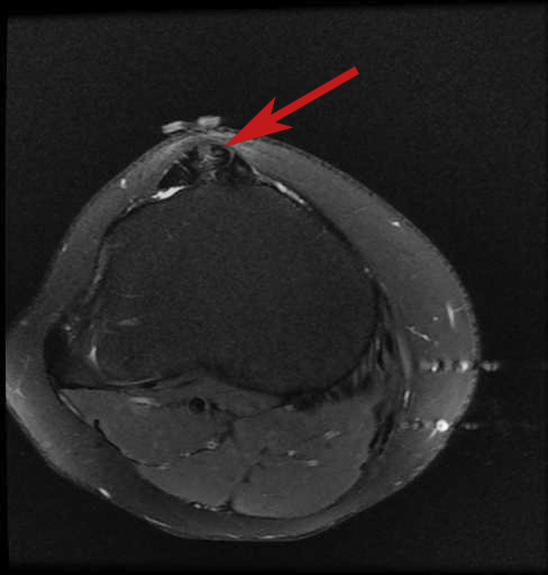
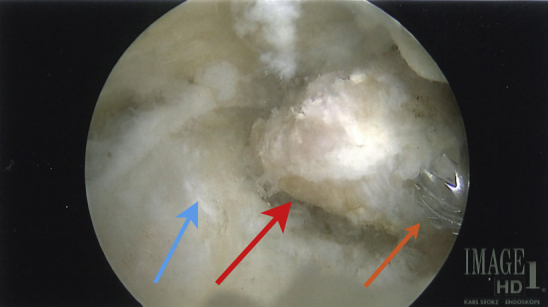
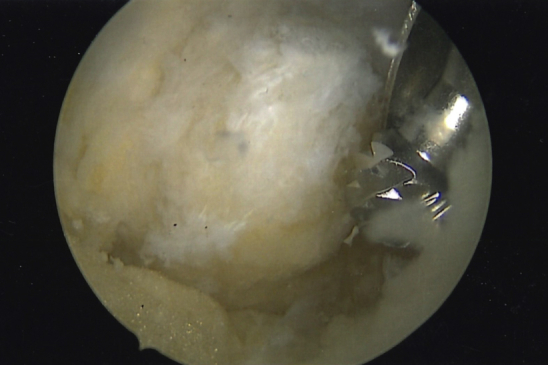
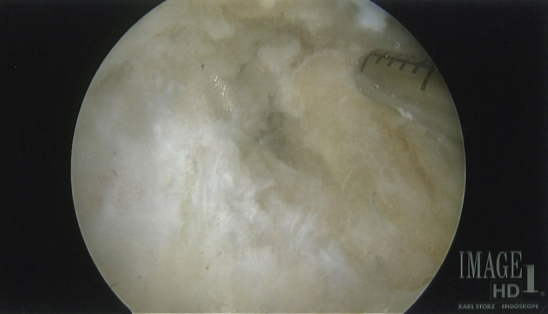
Arthroscopic resection of symptomatic unfused tibial tubercle ossicles causing chronic anterior knee pain due to recalcitrant Osgood-Schlatter disease has been shown to be a reproducible arthroscopic technique. Although a number of other surgical techniques have been described, including ossicle excision and tubercle-plasty, drilling of the tibial tubercle, bone peg insertion to induce fusion, open excision of loose fragments, direct bursoscopic ossicle resection, and closing-wedge tubercle osteotomy, with varied outcomes, this technique offers a minimally invasive approach with low risk. Complications including injury to the patellar tendon and scarring of the anterior fat pad have been previously reported, but this approach can be performed with minimal fat pad debridement and direct visualization of the patellar tendon during all resections. This article presents a technique for arthroscopic resection and debridement of unfused ossicles in patients with chronic anterior knee pain due to Osgood-Schlatter disease by use of minimally invasive arthroscopic techniques that are used in standard knee arthroscopy and should be familiar to most arthroscopists.
© 2022 The Authors.
Figures



Similar articles
-
Osgood-Schlatter Disease: Ossicle Resection and Patellar Tendon Repair in a Symptomatic Adult.Arthrosc Tech. 2024 Jul 9;13(11):103110. doi: 10.1016/j.eats.2024.103110. eCollection 2024 Nov. Arthrosc Tech. 2024. PMID: 39711897 Free PMC article.
-
Arthroscopic Excision of a Huge Ununited Ossicle Due to Osgood-Schlatter Disease in an Adult Patient.J Orthop Case Rep. 2013 Apr-Jun;3(2):4-7. doi: 10.13107/jocr.2250-0685.092. J Orthop Case Rep. 2013. PMID: 27298897 Free PMC article.
-
Arthroscopic excision of an ununited ossicle due to Osgood-Schlatter disease.Arthroscopy. 2008 Sep;24(9):1081-3. doi: 10.1016/j.arthro.2007.03.010. Epub 2007 May 7. Arthroscopy. 2008. PMID: 18760218
-
Treatment of Osgood-Schlatter disease: review of the literature.Musculoskelet Surg. 2017 Dec;101(3):195-200. doi: 10.1007/s12306-017-0479-7. Epub 2017 Jun 7. Musculoskelet Surg. 2017. PMID: 28593576 Review.
-
Apophysitis of the Tibial Tuberosity (Osgood-Schlatter Disease): A Review.Cureus. 2016 Sep 13;8(9):e780. doi: 10.7759/cureus.780. Cureus. 2016. PMID: 27752406 Free PMC article. Review.
Cited by
-
Arthroscopic resection of localized tenosynovial giant cell tumor in the deep infrapatellar bursa: a case report.Croat Med J. 2023 Apr 30;64(2):135-139. doi: 10.3325/cmj.2023.64.135. Croat Med J. 2023. PMID: 37131315 Free PMC article.
-
An MRI-Based Method for the Morphologic Assessment of the Anterior Tibial Tuberosity.J Clin Med. 2024 Nov 3;13(21):6601. doi: 10.3390/jcm13216601. J Clin Med. 2024. PMID: 39518738 Free PMC article.
-
Osgood-Schlatter Disease: Ossicle Resection and Patellar Tendon Repair in a Symptomatic Adult.Arthrosc Tech. 2024 Jul 9;13(11):103110. doi: 10.1016/j.eats.2024.103110. eCollection 2024 Nov. Arthrosc Tech. 2024. PMID: 39711897 Free PMC article.
-
Arthroscopic Tibial Tubercle Osteophyte Debridement and Gout Crystal Clearance for the Treatment of Osgood-Schlatter Disease Complicated With Gout in Patients With Anterior Knee Pain.Arthrosc Tech. 2025 Jan 3;14(5):103369. doi: 10.1016/j.eats.2024.103369. eCollection 2025 May. Arthrosc Tech. 2025. PMID: 40547983 Free PMC article.
-
Bone Infarcts and Tumorigenesis-Is There a Connection? A Mini-Mapping Review.Int J Environ Res Public Health. 2022 Jul 29;19(15):9282. doi: 10.3390/ijerph19159282. Int J Environ Res Public Health. 2022. PMID: 35954639 Free PMC article.
References
-
- Weiler R., Ingram M., Wolman R. 10-Minute consultation. Osgood-Schlatter disease. BMJ. 2021;343:d4534. - PubMed
-
- Ross M.D., Villard D. Disability levels of college-aged men with a history of Osgood-Schlatter disease. J Strength Cond Res. 2003;17:659–663. - PubMed
-
- Pagenstert G., Wurm M., Gehmert S., Egloff C. Reduction osteotomy of the prominent tibial tubercle after Osgood-Schlatter disease. Arthroscopy. 2017;33:1551–1557. - PubMed
-
- Krause B.L., Williams J.P., Catterall A. Natural history of Osgood-Schlatter disease. J Pediatr Orthop. 1990;10:65–68. - PubMed
-
- Gholve P.A., Scher D.M., Khakharia S., Widmann R.F., Green D.W. Osgood Schlatter syndrome. Curr Opin Pediatr. 2007;19:44–50. - PubMed
LinkOut - more resources
Full Text Sources
