

MRI-Based Radiomics Features to Predict Treatment Response to Neoadjuvant Chemotherapy in Locally Advanced Rectal Cancer: A Single Center, Prospective Study
- PMID: 35646677
- PMCID: PMC9133669
- DOI: 10.3389/fonc.2022.801743
MRI-Based Radiomics Features to Predict Treatment Response to Neoadjuvant Chemotherapy in Locally Advanced Rectal Cancer: A Single Center, Prospective Study
Abstract
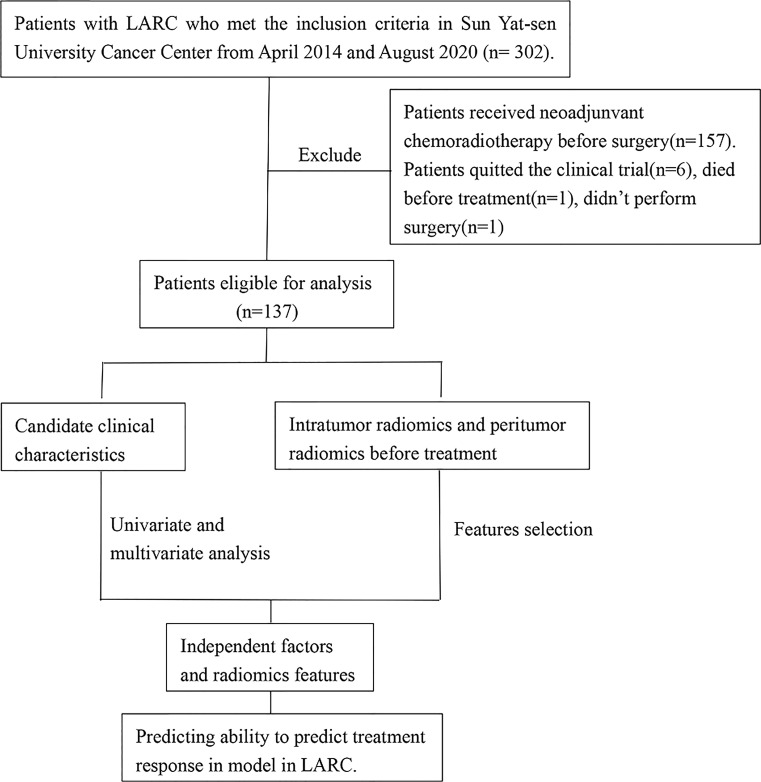
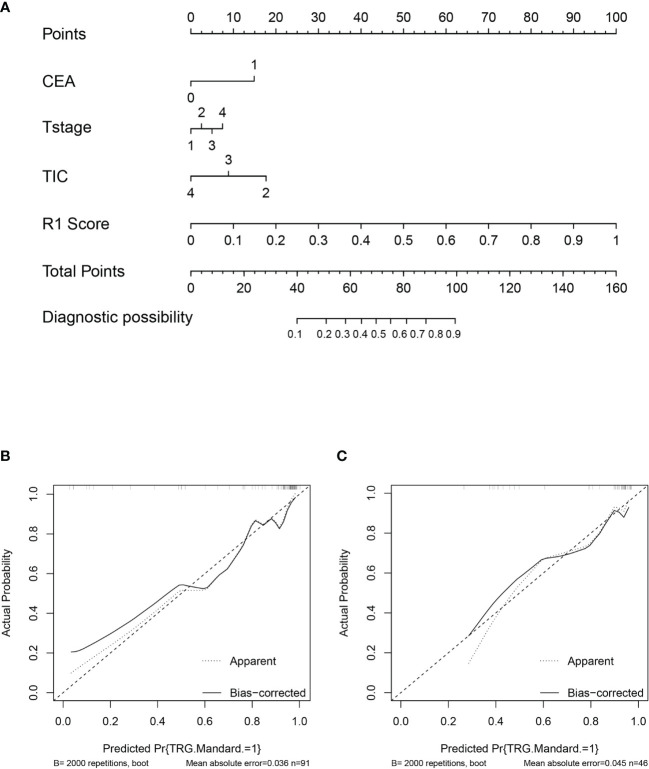
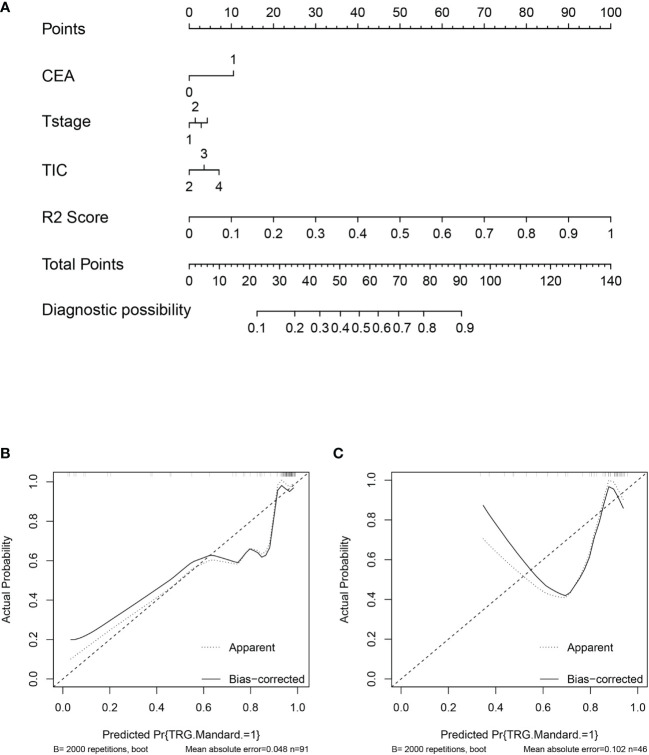
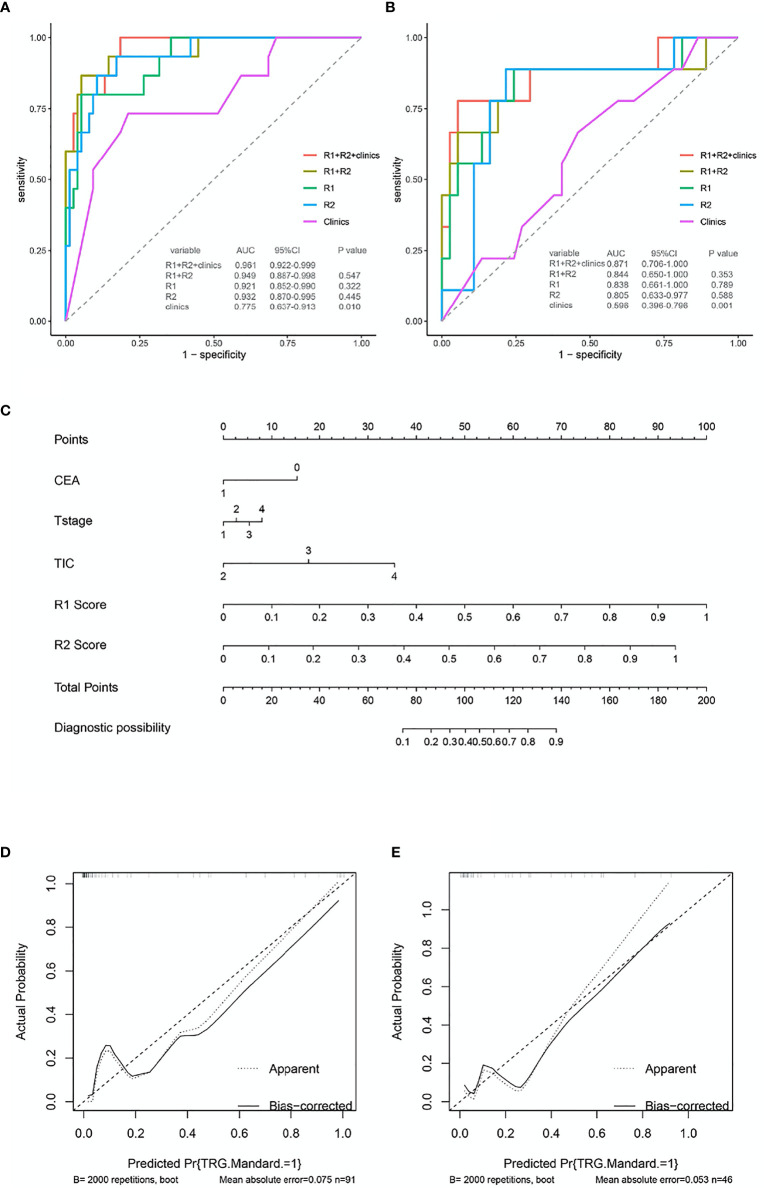
This is a prospective, single center study aimed to evaluate the predictive power of peritumor and intratumor radiomics features assessed using T2 weight image (T2WI) of baseline magnetic resonance imaging (MRI) in evaluating pathological good response to NAC in patients with LARC (including Tany N+ or T3/4a Nany but not T4b). In total, 137 patients with LARC received NAC between April 2014 and August 2020. All patients were undergoing contrast-enhanced MRI and 129 patients contained small field of view (sFOV) sequence which were performed prior to treatment. The tumor regression grade standard was based on pathological response. The training and validation sets (n=91 vs. n=46) were established by random allocation of the patients. Receiver operating characteristic curve (ROC) analysis was applied to estimate the performance of different models based on clinical characteristics and radiomics features obtained from MRI, including peritumor and intratumor features, in predicting treatment response; these effects were calculated using the area under the curve (AUC). The performance and agreement of the nomogram were estimated using calibration plots. In total, 24 patients (17.52%) achieved a complete or near-complete response. For the individual radiomics model in the validation set, the performance of peritumor radiomics model in predicting treatment response yield an AUC of 0.838, while that of intratumor radiomics model is 0.805, which show no statically significant difference between then(P>0.05). The traditional and selective clinical features model shows a poor predictive ability in treatment response (AUC=0.596 and 0.521) in validation set. The AUC of combined radiomics model was improved compared to that of the individual radiomics models in the validation sets (AUC=0.844). The combined clinic-radiomics model yield the highest AUC (0.871) in the validation set, although it did not improve the performance of the radiomics model for predicting treatment response statically (P>0.05). Good agreement and discrimination were observed in the nomogram predictions. Both peritumor and intratumor radiomics features performed similarly in predicting a good response to NAC in patients with LARC. The clinic-radiomics model showed the best performance in predicting treatment response.
Keywords: magnetic resonance imaging radiomics; neoadjuvant chemotherapy; nomogram; rectal cancer; treatment response.
Copyright © 2022 Chen, Xie, Li, Jiang, Xiong, Tang, Lin, Li and Cai.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Bahadoer RR, Dijkstra EA, van Etten B, Marijnen CAM, Putter H, Kranenbarg EM, et al. Short-Course Radiotherapy Followed by Chemotherapy Before Total Mesorectal Excision (TME) Versus Preoperative Chemoradiotherapy, TME, and Optional Adjuvant Chemotherapy in Locally Advanced Rectal Cancer (RAPIDO): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol (2021) 22(1):29–42. doi: 10.1016/S1470-2045(20)30555-6 - DOI - PubMed
-
- Habr-Gama A, Perez RO, Nadalin W, Sabbaga J, Ribeiro U, Jr, Silva e Sousa AH, Jr, et al. Operative Versus Nonoperative Treatment for Stage 0 Distal Rectal Cancer Following Chemoradiation Therapy: Long-Term Results. Ann Surg (2004) 240(4):711–717; discussion 717-718. doi: 10.1097/01.sla.0000141194.27992.32 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous