

Anatomical Computerized Exploration to Excise Malignancies in Deep Facial Compartments: An Advanced Virtual Reality Protocol for a Tailored Surgical Approach
- PMID: 35646710
- PMCID: PMC9137398
- DOI: 10.3389/fonc.2022.875990
Anatomical Computerized Exploration to Excise Malignancies in Deep Facial Compartments: An Advanced Virtual Reality Protocol for a Tailored Surgical Approach
Abstract
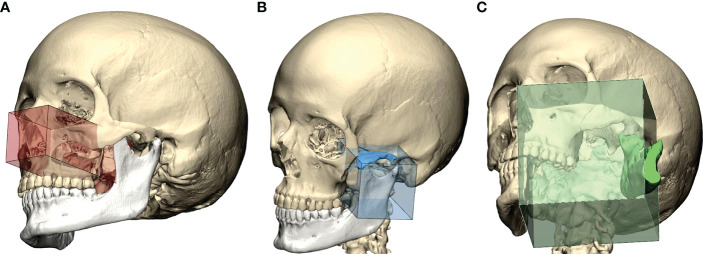
Objective/hypothesis: This study describes the design and application of a novel advanced protocol for virtual three-dimensional anatomical reconstruction of the deep facial compartments, aiming to improve the preoperative understanding and the intraoperative assistance in complex resective surgeries performed for malignant diseases which extend in complex spaces, including the pterygomaxillopalatine fossa, the masticator space, and the infratemporal fossa.
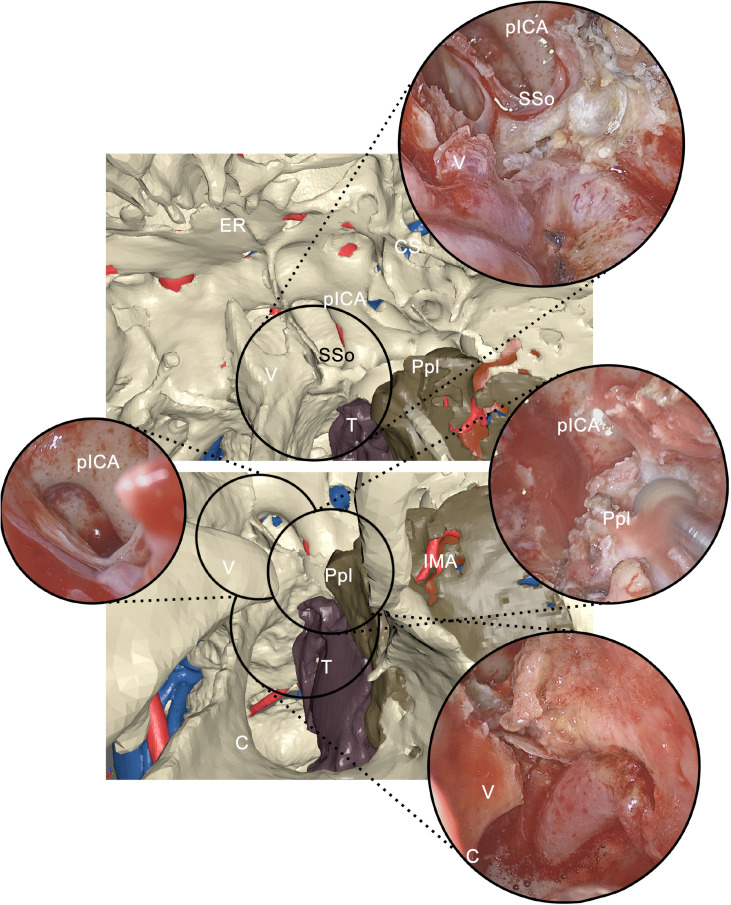
Methods: This study is a non-profit, retrospective, and single-institution case series. The authors clearly describe in detail imaging acquisition protocols which are suitable to segment each target, and a multilayer reconstruction technique is presented to simulate anatomical structures, with particular focus on vascular networks. Virtual surgical planning techniques are individually designed for each case to provide the most effective access to the deep facial compartments. Intraoperative guidance systems, including navigation and virtual endoscopy, are presented, and their role is analyzed.
Results: The study included seven patients with malignant disease located in the deep facial compartments requiring radical resection, and all patients underwent successful application of the protocol. All lesions, except one, were subject to macroscopically radical resection. Vascular structures were identified with overall reconstruction rates superior to 90% for major caliber vessels. Prominent landmarks for virtual endoscopy were identified for each case.
Conclusions: Virtual surgical planning and multilayer anatomical reconstruction are valuable methods to implement for surgeries in deep facial compartments, providing the surgeon with improved understanding of the preoperative condition and intraoperative guidance in critical phases for both open and endoscopic phases. Such techniques allow to tailor each surgical access, limiting morbidity to strictly necessary approaches to reach the disease target.
Keywords: 3D vessels; deep facial compartments; navigation; virtual endoscopy; virtual surgical planning.
Copyright © 2022 Tel, Bagatto, Costa, Sembronio and Robiony.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






Similar articles
-
Exploring Deep Cervical Compartments in Head and Neck Surgical Oncology through Augmented Reality Vision: A Proof of Concept.J Clin Med. 2023 Oct 20;12(20):6650. doi: 10.3390/jcm12206650. J Clin Med. 2023. PMID: 37892787 Free PMC article.
-
The Transantral Endoscopic Approach: A Portal for Masses of the Inferior Orbit-Improving Surgeons' Experience Through Virtual Endoscopy and Augmented Reality.Front Surg. 2021 Aug 23;8:715262. doi: 10.3389/fsurg.2021.715262. eCollection 2021. Front Surg. 2021. PMID: 34497829 Free PMC article.
-
Early Experience With Virtual and Synchronized Augmented Reality Platform for Preoperative Planning and Intraoperative Navigation: A Case Series.Oper Neurosurg. 2021 Sep 15;21(4):189-196. doi: 10.1093/ons/opab188. Oper Neurosurg. 2021. PMID: 34171909 Free PMC article.
-
Virtual Reality Exploration and Planning for Precision Colorectal Surgery.Dis Colon Rectum. 2018 Jun;61(6):719-723. doi: 10.1097/DCR.0000000000001077. Dis Colon Rectum. 2018. PMID: 29722730
-
The application of virtual reality and augmented reality in Oral & Maxillofacial Surgery.BMC Oral Health. 2019 Nov 8;19(1):238. doi: 10.1186/s12903-019-0937-8. BMC Oral Health. 2019. PMID: 31703708 Free PMC article. Review.
Cited by
-
Researching the application of virtual reality in medical education: one-year follow-up of a randomized trial.BMC Med Educ. 2023 Jan 3;23(1):3. doi: 10.1186/s12909-022-03992-6. BMC Med Educ. 2023. PMID: 36597093 Free PMC article. Clinical Trial.
-
Exploring Deep Cervical Compartments in Head and Neck Surgical Oncology through Augmented Reality Vision: A Proof of Concept.J Clin Med. 2023 Oct 20;12(20):6650. doi: 10.3390/jcm12206650. J Clin Med. 2023. PMID: 37892787 Free PMC article.
-
Double osseous flaps for simultaneous midfacial and mandible reconstruction: Automation in surgical complexity within an entirely computerized workflow.Front Oncol. 2023 Feb 3;13:1103104. doi: 10.3389/fonc.2023.1103104. eCollection 2023. Front Oncol. 2023. PMID: 36816944 Free PMC article.
-
Complex Craniofacial Cases through Augmented Reality Guidance in Surgical Oncology: A Technical Report.Diagnostics (Basel). 2024 May 27;14(11):1108. doi: 10.3390/diagnostics14111108. Diagnostics (Basel). 2024. PMID: 38893634 Free PMC article.
-
Adverse Effects Associated with Dermal Filler Treatments: Part II Vascular Complication.Diagnostics (Basel). 2024 Jul 18;14(14):1555. doi: 10.3390/diagnostics14141555. Diagnostics (Basel). 2024. PMID: 39061692 Free PMC article. Review.
References
-
- Javan R, Rao A, Jeun BS, Herur-Raman A, Singh N, Heidari P. From CT to 3D Printed Models, Serious Gaming, and Virtual Reality: Framework for Educational 3d Visualization of Complex Anatomical Spaces From Within—the Pterygopalatine Fossa. J Digit Imaging (2020) 33:776–91. doi: 10.1007/s10278-019-00315-y - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources