

Valproic Acid Reduces Neuroinflammation to Provide Retinal Ganglion Cell Neuroprotection in the Retina Axotomy Model
- PMID: 35646919
- PMCID: PMC9135180
- DOI: 10.3389/fcell.2022.903436
Valproic Acid Reduces Neuroinflammation to Provide Retinal Ganglion Cell Neuroprotection in the Retina Axotomy Model
Abstract
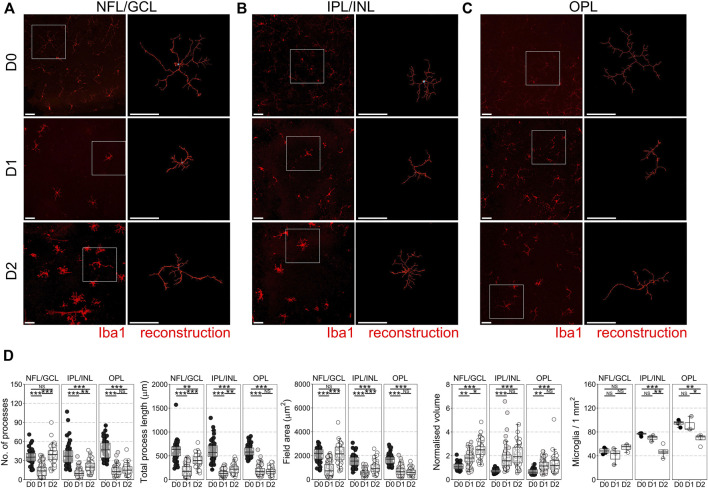
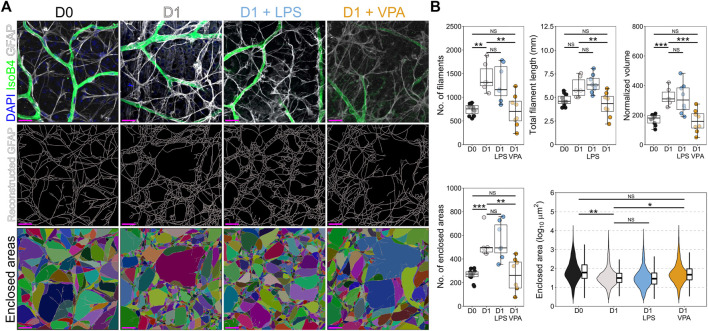
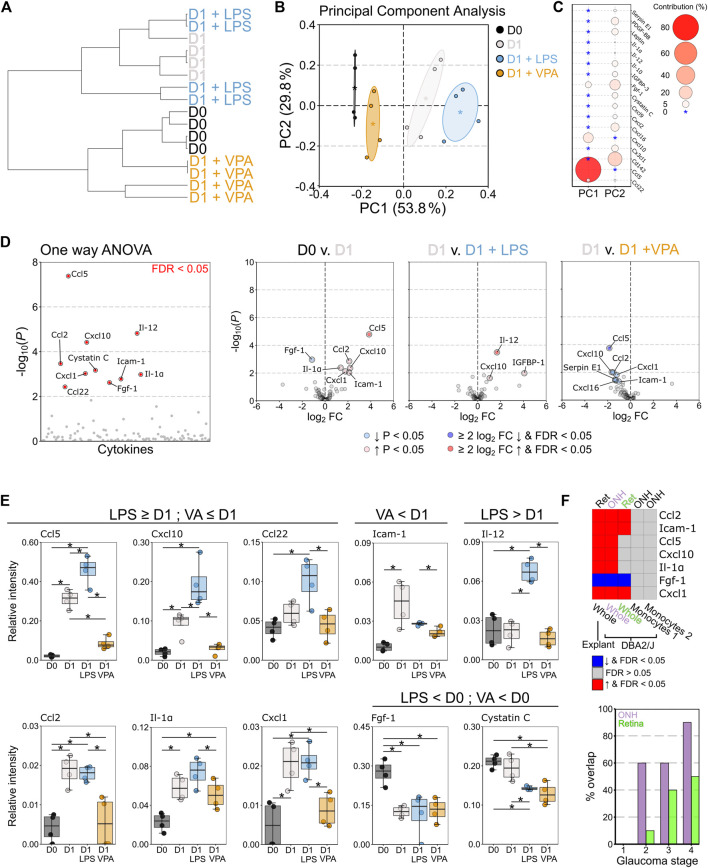
Neuroinflammation is a critical and targetable pathogenic component of neurodegenerative diseases, including glaucoma, the leading cause of irreversible blindness. Valproic acid has previously been demonstrated to reduce neuroinflammation and is neuroprotective in a number of experimental settings. To determine whether valproic acid can limit retinal neuroinflammation and protect retinal neurons we used an ex vivo retina explant (axotomy) model to isolate resident glial responses from blood-derived monocytes. Neuroinflammatory status was defined using high resolution confocal imaging with 3D morphological reconstruction and cytokine protein arrays. Valproic acid significantly reduced microglia and astrocyte morphological changes, consistent with a reduction in pro-inflammatory phenotypes. Cytokine profiling demonstrated that valproic acid significantly attenuated or prevented expression of pro-inflammatory cytokines in injured retina. This identifies that the retinal explant model as a useful tool to explore resident neuroinflammation in a rapid timescale whilst maintaining a complex system of cell interactions and valproic acid as a useful drug to further explore anti-neuroinflammatory strategies in retinal disease.
Keywords: astrocyte; glaucoma; microglia; neuroinflammation; retina.
Copyright © 2022 Tribble, Kastanaki, Uslular, Rutigliani, Enz and Williams.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
CHOP deletion and anti-neuroinflammation treatment with hesperidin synergistically attenuate NMDA retinal injury in mice.Exp Eye Res. 2021 Dec;213:108826. doi: 10.1016/j.exer.2021.108826. Epub 2021 Nov 6. Exp Eye Res. 2021. PMID: 34752818
-
Transgenic inhibition of astroglial NF-κB restrains the neuroinflammatory and neurodegenerative outcomes of experimental mouse glaucoma.J Neuroinflammation. 2020 Aug 28;17(1):252. doi: 10.1186/s12974-020-01930-1. J Neuroinflammation. 2020. PMID: 32859212 Free PMC article.
-
Evaluation of neuroprotective and immunomodulatory properties of mesenchymal stem cells in an ex vivo retinal explant model.J Neuroinflammation. 2022 Mar 2;19(1):63. doi: 10.1186/s12974-022-02418-w. J Neuroinflammation. 2022. PMID: 35236378 Free PMC article.
-
Neuroinflammation, Microglia and Implications for Retinal Ganglion Cell Survival and Axon Regeneration in Traumatic Optic Neuropathy.Front Immunol. 2022 Mar 4;13:860070. doi: 10.3389/fimmu.2022.860070. eCollection 2022. Front Immunol. 2022. PMID: 35309305 Free PMC article. Review.
-
Neuroprotection, Growth Factors and BDNF-TrkB Signalling in Retinal Degeneration.Int J Mol Sci. 2016 Sep 20;17(9):1584. doi: 10.3390/ijms17091584. Int J Mol Sci. 2016. PMID: 27657046 Free PMC article. Review.
Cited by
-
Retinoprotective compounds, current efficacy, and future prospective.Neural Regen Res. 2023 Dec;18(12):2619-2622. doi: 10.4103/1673-5374.373662. Neural Regen Res. 2023. PMID: 37449599 Free PMC article. Review.
-
Pyrroloquinoline quinone drives ATP synthesis in vitro and in vivo and provides retinal ganglion cell neuroprotection.Acta Neuropathol Commun. 2023 Sep 8;11(1):146. doi: 10.1186/s40478-023-01642-6. Acta Neuropathol Commun. 2023. PMID: 37684640 Free PMC article.
-
Oxidative Stress: A Suitable Therapeutic Target for Optic Nerve Diseases?Antioxidants (Basel). 2023 Jul 20;12(7):1465. doi: 10.3390/antiox12071465. Antioxidants (Basel). 2023. PMID: 37508003 Free PMC article. Review.
-
Role of glia in delirium: proposed mechanisms and translational implications.Mol Psychiatry. 2025 Mar;30(3):1138-1147. doi: 10.1038/s41380-024-02801-4. Epub 2024 Oct 27. Mol Psychiatry. 2025. PMID: 39463449 Free PMC article. Review.
-
Epigenetics in Glaucoma.Medicina (Kaunas). 2024 May 29;60(6):905. doi: 10.3390/medicina60060905. Medicina (Kaunas). 2024. PMID: 38929522 Free PMC article. Review.
References
-
- Bates D., Mächler M., Bolker B., Walker S. (2015). Fitting Linear Mixed-Effects Models Using Lme4. J. Stat. Softw. 67 (1), 48. 10.18637/jss.v067.i01 - DOI
LinkOut - more resources
Full Text Sources