

Poor Outcomes in Patients With Transplant Glomerulopathy Independent of Banff Categorization or Therapeutic Interventions
- PMID: 35646957
- PMCID: PMC9133540
- DOI: 10.3389/fmed.2022.889648
Poor Outcomes in Patients With Transplant Glomerulopathy Independent of Banff Categorization or Therapeutic Interventions
Abstract
Background: Transplant glomerulopathy (TG) may indicate different disease entities including chronic AMR (antibody-mediated rejection). However, AMR criteria have been frequently changed, and long-term outcomes of allografts with AMR and TG according to Banff 2017 have rarely been investigated.
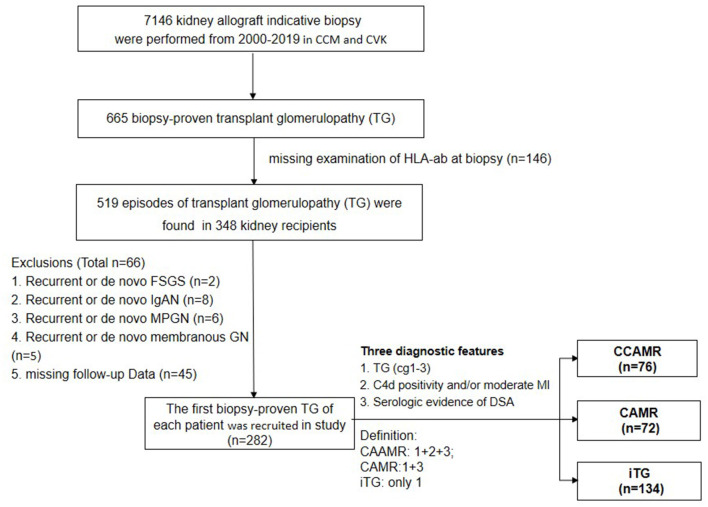
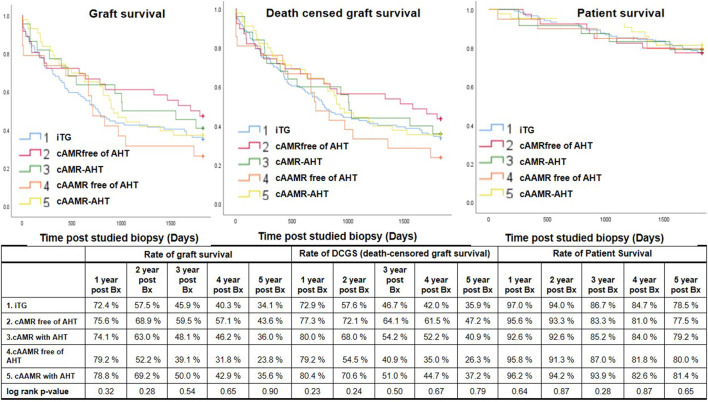
Methods: 282 kidney allograft recipients with biopsy-proven TG were retrospectively investigated and diagnosed according to Banff'17 criteria: chronic AMR (cAMR, n = 72), chronic active AMR (cAAMR, n = 76) and isolated TG (iTG, n = 134). Of which 25/72 (34.7%) patients of cAMR group and 46/76 (60.5%) of cAAMR group were treated with antihumoral therapy (AHT).
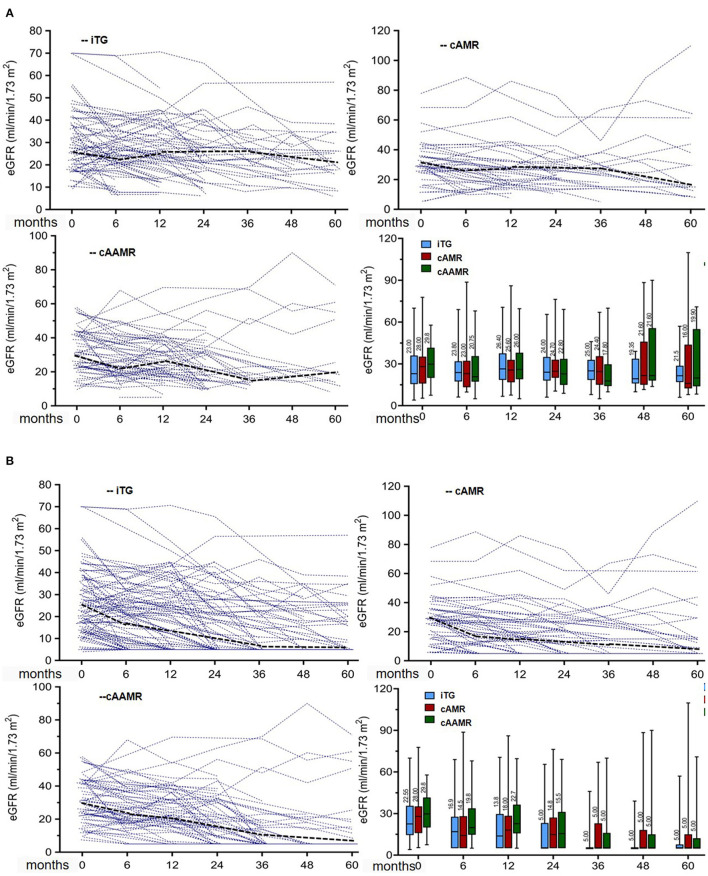
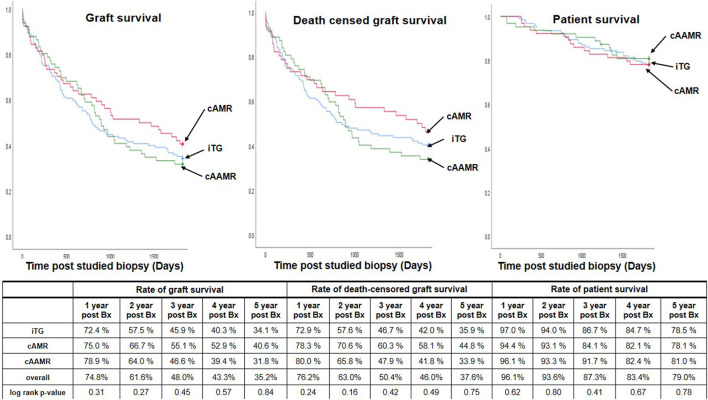
Results: Up to 5 years after indication biopsy, no statistically significant differences were detected among iTG, cAMR and cAAMR groups in annual eGFR decline (-3.0 vs. -2.0 vs. -2.8 ml/min/1.73 m2 per year), 5-year median eGFR (21.5 vs. 16.0 vs. 20.0 ml/min/1.73 m2), 5-year graft survival rates (34.1 vs. 40.6 vs. 31.8%) as well as urinary protein excretion during follow-up. In addition, cAMR and cAAMR patients treated with AHT had similar graft and patient survival rates in comparison with those free of AHT, and similar comparing with iTG group. The TG scores were not associated with 5-year postbiopsy graft failure; whereas the patients with higher scores of chronic allograft scarring (by mm-, ci- and ct-lesions) had significantly lower graft survival rates than those with mild scores. The logistic-regression analysis demonstrated that Banff mm-, ah-, t-, ci-, ct-lesions and the eGFR level at biopsy were associated with 5-year graft failure.
Conclusions: The occurrence of TG is closely associated with graft failure independent of disease categories and TG score, and the long-term clinical outcomes were not influenced by AHT. The Banff lesions indicating progressive scarring might be better suited to predict an unfavorable outcome.
Keywords: antihumoral therapy; chronic antibody-mediated rejection; graft survival; kidney transplantation; transplant glomerulopathy.
Copyright © 2022 Wu, Schmidt, López del Moral, Osmanodja, Lachmann, Halleck, Choi, Bachmann, Ronicke, Duettmann, Naik, Schrezenmeier, Rudolph and Budde.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous