

Clinical Relevance of the LVEDD and LVESD Trajectories in HF Patients With LVEF < 35
- PMID: 35646999
- PMCID: PMC9136034
- DOI: 10.3389/fmed.2022.846361
Clinical Relevance of the LVEDD and LVESD Trajectories in HF Patients With LVEF < 35
Abstract
Background: Certain variables reportedly are associated with a change in left ventricular ejection fraction (LVEF) in heart failure (HF) with reduced ejection fraction (HFrEF). However, literature describing the association between the recovery potential of LVEF and parameters of ventricular remodeling in echocardiography remains sparse.
Methods: We recruited 2,148 HF patients with LVEF < 35%. All patients underwent at least two echocardiographic images. The study aimed to compare LVEF alterations and their association with patient characteristics and echocardiographic findings.
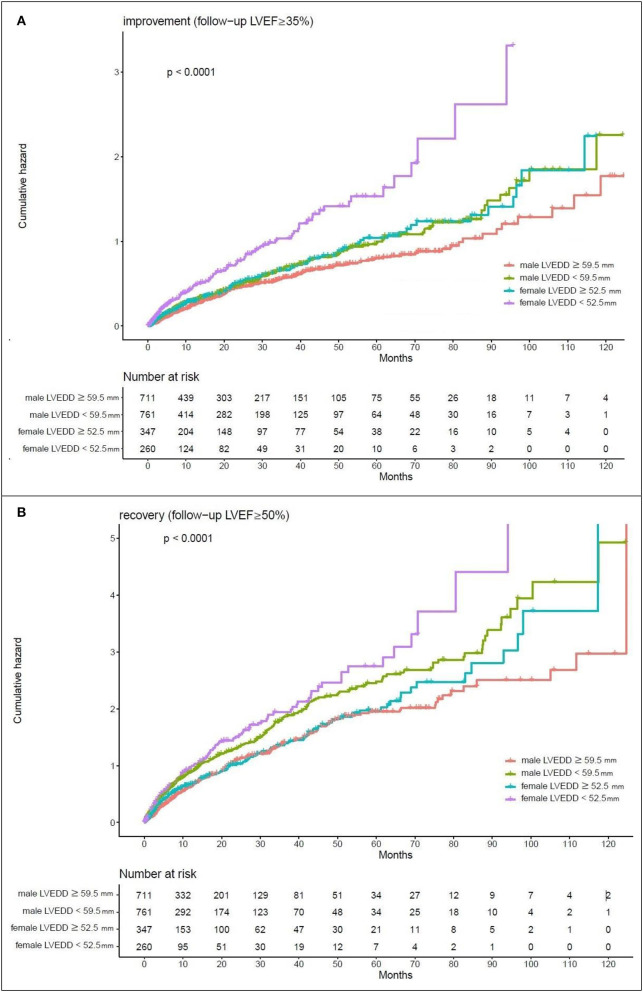
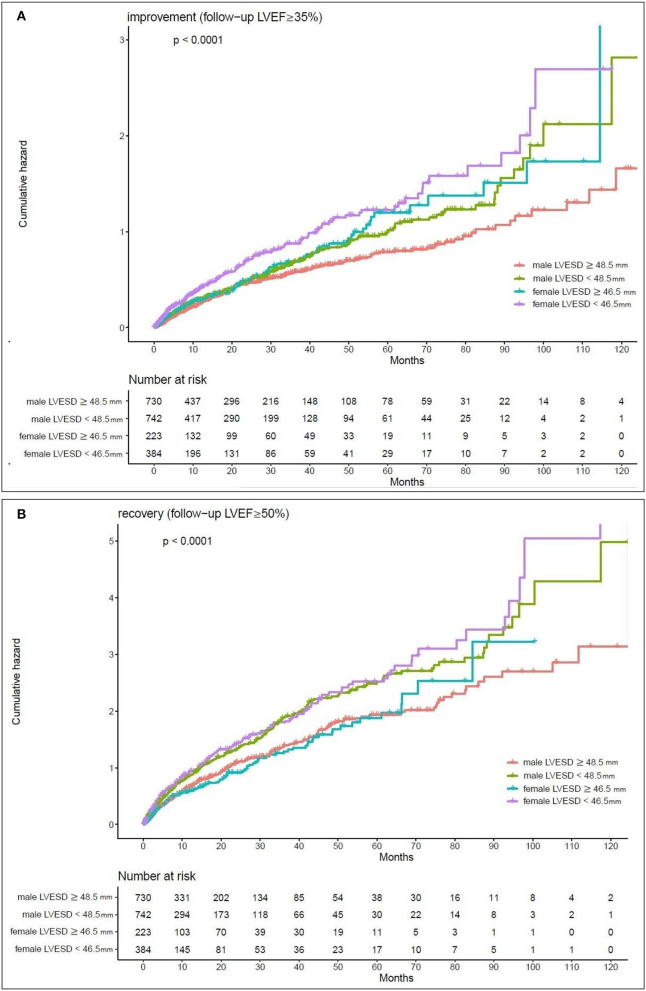
Results: Patients with "recovery" of LVEF (follow-up LVEF ≥ 50%) were less likely to have prior myocardial infarction (MI), had a higher prevalence of atrial fibrillation (Af), were less likely to have diabetes and hypertension, and had a smaller left atrium (LA) diameter, left ventricular end-diastolic diameter (LVEDD) and left ventricular end-systolic diameter (LVESD), both in crude and in adjusted models (adjustment for age and sex). LVEDD cutoff values of 59.5 mm in men and 52.5 mm in women and LVESD cutoff values of 48.5 mm in men and 46.5 mm in women showed a year-to-year increase in the rate of recovery (follow-up LVEF ≥ 50%)/improvement (follow-up LVEF ≥ 35%), p-value < 0.05 in Kaplan-Meier estimates of the cumulative hazard curves.
Conclusions: Our study shows that LVEDD and LVESD increments in echocardiography can be predictors of changes in LVEF in in HF patients with LVEF < 35%. They may be used to identify patients who require more aggressive therapeutic interventions.
Keywords: changes in ejection fraction; ejection fraction; heart failure with reduced ejection fraction (HFrEF); left ventricle end diastolic dimension (LVEDD); left ventricle end systolic dimension (LVESD).
Copyright © 2022 Chen, Hsing, Chao, Cheng, Lin, Lin and Fang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson T, Flegal K, et al. . American Heart Association Statistics Committee and Stroke Statistics Subcommittee: Heart disease and stroke statistics-2009 update: a report from the American heart association statistics committee and stroke statistics subcommittee. Circulation. (2009) 119:480–6. 10.1161/CIRCULATIONAHA.108.191259 - DOI - PubMed
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, et al. . Corrigendum to: 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2021) 42:3599–726. 10.1093/eurheartj/ehab670 - DOI - PubMed
-
- Chioncel O, Lainscak M, Seferovic PM, Anker SD, Crespo-Leiro MG, Harjola VP, et al. . Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. (2017) 19:1574–85. 10.1002/ejhf.813 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous