

Successful multimodality treatment of metastatic gallbladder cancer: A case report and review of literature
- PMID: 35647145
- PMCID: PMC9100720
- DOI: 10.12998/wjcc.v10.i12.3856
Successful multimodality treatment of metastatic gallbladder cancer: A case report and review of literature
Abstract
Background: Gallbladder cancer is the most common malignant tumor in the biliary system, and it is characterized by high aggressiveness and an extremely poor prognosis. Current treatment for advanced gallbladder cancer remains unsatisfactory. Here, we report a patient with advanced gallbladder cancer who was cured by multidisciplinary treatment.
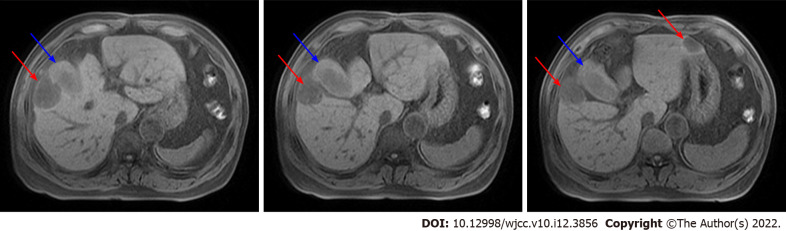
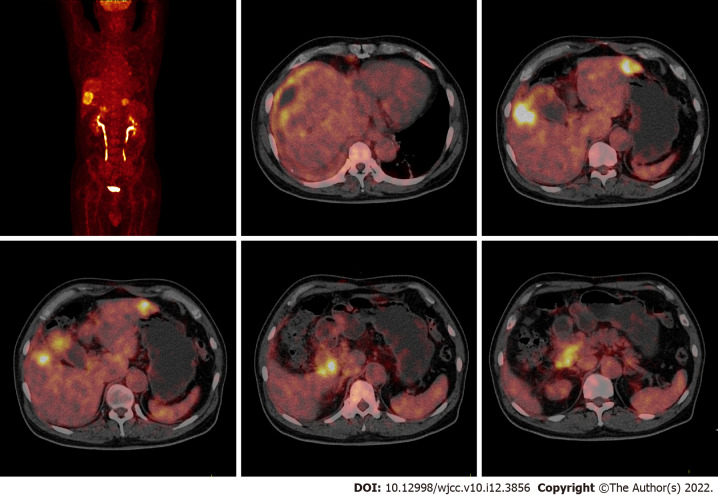
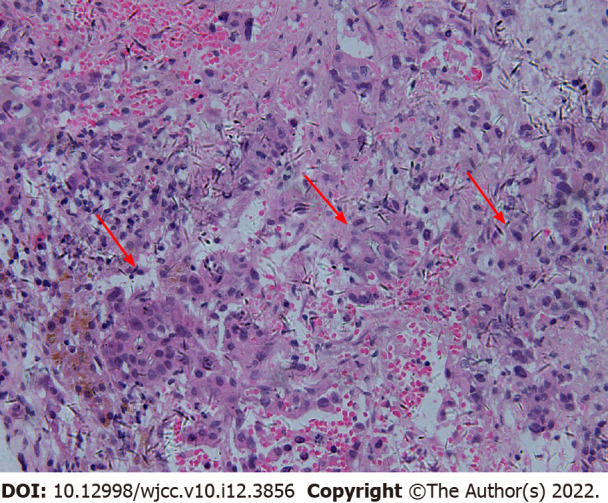
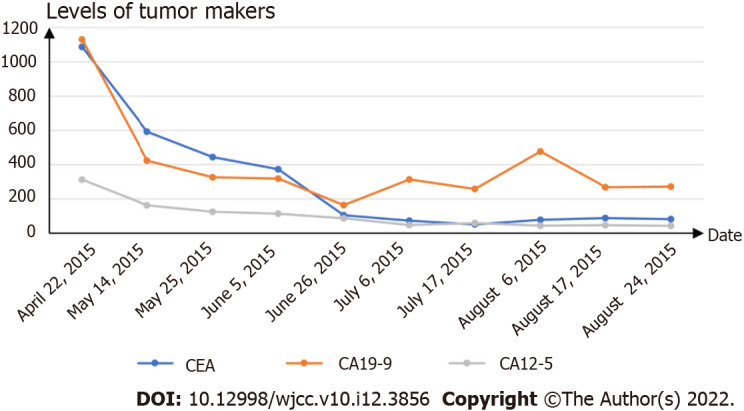
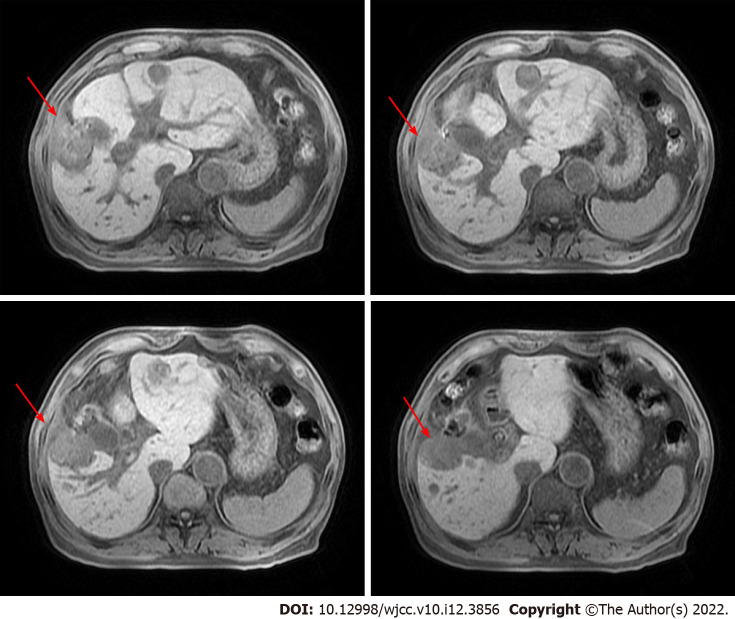
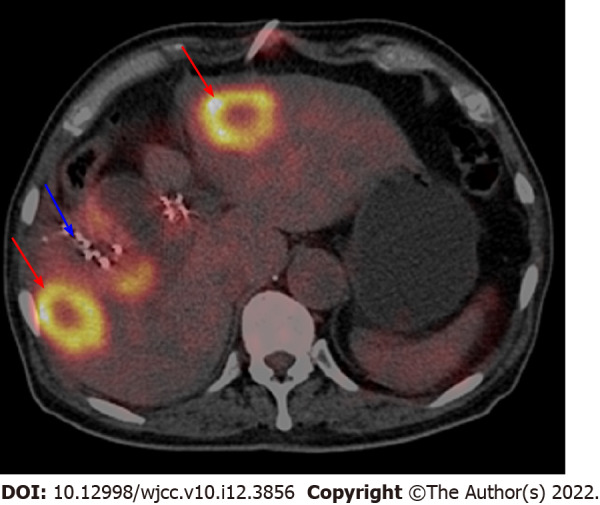
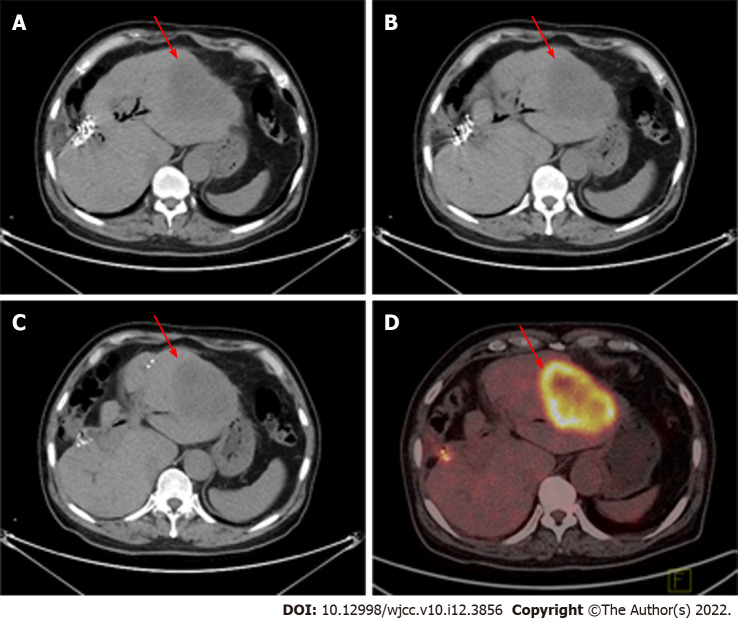
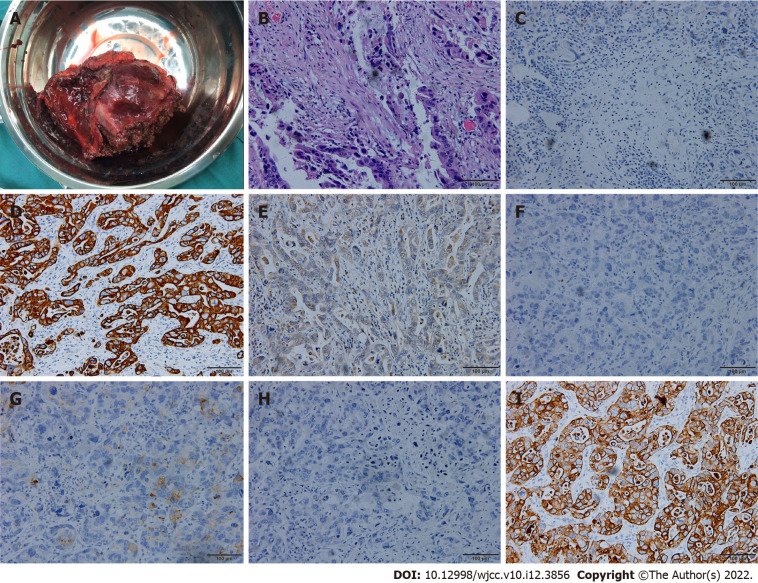
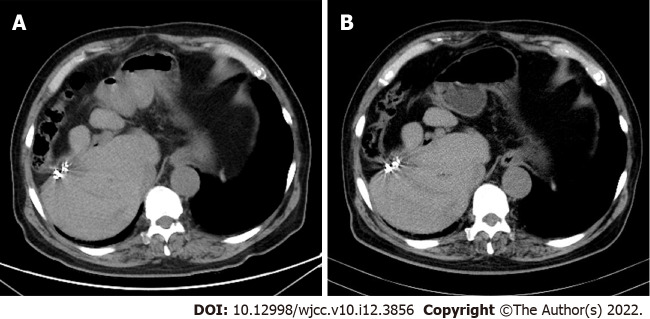
Case summary: A 73-year-old male presented to our hospital with right abdominal pain for 3 d and was diagnosed with stage IVB gallbladder cancer with multiple liver metastases, peritoneum metastasis, diaphragm metastasis and lymph node metastases. The patient initially received chemotherapy, targeted therapy, 125I seed implantation and immunotherapy, as there were no specific indications for radical surgery. During these palliative therapies, the level of tumor markers gradually decreased but remained higher than the normal level, lymph node metastases gradually disappeared, and liver metastasis was gradually limited to the left liver. Finally, the patient received radical surgery with left hepatectomy, radical lymphadenectomy and partial diaphragmatic resection. To date, the patient has survived for more than six years posttreatment, the levels of tumor markers are normal, and imaging examinations show no signs of tumor recurrence.
Conclusion: Currently, the prognosis of advanced gallbladder cancer remains unsatisfactory. A single treatment method is not sufficient for patients with advanced gallbladder cancer. Multidisciplinary individualized treatment is essential and should be utilized for advanced gallbladder cancer patients to further improve prognosis.
Keywords: Advanced gallbladder cancer; Case report; Long-term survival; Multidisciplinary treatment.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
Similar articles
-
"Extended" radical cholecystectomy for gallbladder cancer: long-term outcomes, indications and limitations.World J Gastroenterol. 2012 Sep 14;18(34):4736-43. doi: 10.3748/wjg.v18.i34.4736. World J Gastroenterol. 2012. PMID: 23002343 Free PMC article.
-
Mode of tumor spread and surgical strategy in gallbladder carcinoma.Langenbecks Arch Surg. 2002 Oct;387(5-6):222-8. doi: 10.1007/s00423-002-0318-6. Epub 2002 Oct 2. Langenbecks Arch Surg. 2002. PMID: 12410358
-
Long-term survival of a recurrent gallbladder carcinoma patient with lymph node and peritoneal metastases after multidisciplinary treatments: a case report.Surg Case Rep. 2016 Dec;2(1):12. doi: 10.1186/s40792-016-0135-8. Epub 2016 Feb 11. Surg Case Rep. 2016. PMID: 26943688 Free PMC article.
-
[Significance of resecting the head of the pancreas for the treatment of gallbladder cancer from the perspective of surgical results and mode of lymph node metastasis].Nihon Geka Gakkai Zasshi. 2002 Aug;103(8):557-63. Nihon Geka Gakkai Zasshi. 2002. PMID: 12229158 Review. Japanese.
-
Rare Mixed Adenoneuroendocrine Carcinoma of the Gallbladder: Case Report and Review of Literature.Am J Case Rep. 2021 May 4;22:e929511. doi: 10.12659/AJCR.929511. Am J Case Rep. 2021. PMID: 33945521 Free PMC article. Review.
Cited by
-
Predictive and prognostic models and visualizations of distant metastasis in gallbladder cancer.Medicine (Baltimore). 2025 Jul 18;104(29):e43369. doi: 10.1097/MD.0000000000043369. Medicine (Baltimore). 2025. PMID: 40696595 Free PMC article.
References
-
- Weaver AJ, Stafford R, Hale J, Denning D, Sanabria JR GBD Collaborators. Geographical and Temporal Variation in the Incidence and Mortality of Hepato-Pancreato-Biliary Primary Malignancies:1990-2017. J Surg Res. 2020;245:89–98. - PubMed
-
- Zaidi MY, Maithel SK. Updates on Gallbladder Cancer Management. Curr Oncol Rep. 2018;20:21. - PubMed
-
- Hickman L, Contreras C. Gallbladder Cancer: Diagnosis, Surgical Management, and Adjuvant Therapies. Surg Clin North Am. 2019;99:337–355. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
