

Oral anticoagulation versus antiplatelet therapy for secondary stroke prevention in patients with embolic stroke of undetermined source: A systematic review and meta-analysis
- PMID: 35647310
- PMCID: PMC9134773
- DOI: 10.1177/23969873221076971
Oral anticoagulation versus antiplatelet therapy for secondary stroke prevention in patients with embolic stroke of undetermined source: A systematic review and meta-analysis
Erratum in
-
ERRATUM to Oral anticoagulation versus antiplatelet therapy for secondary stroke prevention in patients with embolic stroke of undetermined source: A systematic review and meta-analysis.Eur Stroke J. 2023 Mar;8(1):408. doi: 10.1177/23969873221133919. Epub 2022 Oct 26. Eur Stroke J. 2023. PMID: 37021151 Free PMC article.
Abstract
Purpose: We performed a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the efficacy and safety of direct oral anticoagulation (DOAC) compared with antiplatelet therapy for secondary stroke prevention in adult patients with embolic stroke of undetermined source (ESUS).
Method: We searched major databases (Embase, MEDLINE, CINAHL, CENTRAL, and Web of Science) for RCTs published until March 2021. The primary outcome was recurrent stroke, and the main safety outcomes were major bleeding and clinically relevant non-major bleeding (CRNB). We assessed risk of bias using the Cochrane Risk of Bias tool. We used a random-effects model to determine pooled risk ratios and 95% confidence intervals in the datasets and key subgroups.
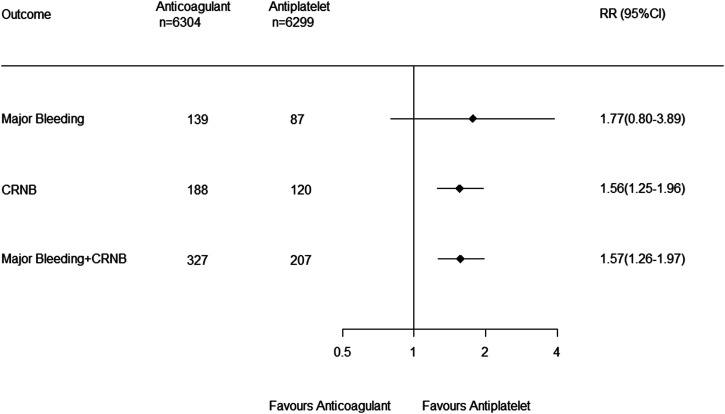
Findings: Our search identified two RCTs, involving a total of 12,603 patients with ESUS. Anticoagulation with dabigatran or rivaroxaban compared with aspirin did not reduce the risk of recurrent stroke (RR, 0.96 [0.76-1.20]) or increase major bleeding (RR, 1.77 [0.80-3.89]) but significantly increased the composite of major or clinically relevant non-major bleeding (RR, 1.57 [1.26-1.97]). Prespecified subgroup analysis demonstrated consistent results according to age and sex. Additional post-hoc subgroup analyses demonstrated consistent results according to prior stroke and presence of a patent foramen ovale but suggested that DOACs reduced recurrent stroke in patients with an estimated glomerular filtration rate (eGFR) <50 and 50-80 ml/min but not in those with eGFR >80 ml/min (interaction P = 0.0234).
Discussion/conclusion: Direct oral anticoagulations are not more effective than aspirin in preventing stroke recurrence in patients with ESUS and increase bleeding.
Registration: PROSPERO ID: CRD42019138593.
Keywords: Anticoagulation; antiplatelet; embolic stroke of undetermined source; prevention; stroke.
© European Stroke Organisation 2022.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In the last 3 years, HCD received honoraria for participation in clinical trials, contribution to advisory boards or oral presentations from: Abbott, BMS, Boehringer Ingelheim, Daiichi-Sankyo, Novo-Nordisk, Pfizer, Portola, and WebMD Global. Financial support for research projects was provided by Boehringer Ingelheim. HCD received research grants from the German Research Council (DFG), German Ministry of Education and Research (BMBF), European Union, NIH, Bertelsmann Foundation, and Heinz-Nixdorf Foundation. JWE has received honoraria and/or research support from Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi-Sankyo, Janssen, Pfizer, Portola, and WebMD Global.
Figures



References
-
- Meschia JF, Brott T. Ischaemic stroke. Eur J Neurol 2018; 25: 35–40. - PubMed
-
- Yaghi S, Bernstein RA, Passman R, et al. Cryptogenic stroke. Circ Res 2017; 120: 527–540. - PubMed
-
- Hart RG, Diener H-C, Coutts SB, et al. Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol 2014; 13: 429–438. - PubMed
-
- Hart RG, Sharma M, Mundl H, et al. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. N Engl J Med 2018; 378: 2191–2201. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
