

Pressor therapy in acute ischaemic stroke: an updated systematic review
- PMID: 35647316
- PMCID: PMC9134777
- DOI: 10.1177/23969873221078136
Pressor therapy in acute ischaemic stroke: an updated systematic review
Erratum in
-
ERRATUM to Pressor therapy in acute ischaemic stroke: An updated systematic review.Eur Stroke J. 2023 Mar;8(1):409. doi: 10.1177/23969873221133920. Epub 2022 Oct 26. Eur Stroke J. 2023. PMID: 37021201 Free PMC article.
Abstract
Background: Low blood pressure (BP) in acute ischaemic stroke (AIS) is associated with poor functional outcome, death, or severe disability. Increasing BP might benefit patients with post-stroke hypotension including those with potentially salvageable ischaemic penumbra. This updated systematic review considers the present evidence regarding the use of vasopressors in AIS.
Methods: We searched the Cochrane Database of Systematic Reviews, MEDLINE, EMBASE and trial databases using a structured search strategy. We examined reference lists of relevant publications for additional studies examining BP elevation in AIS.
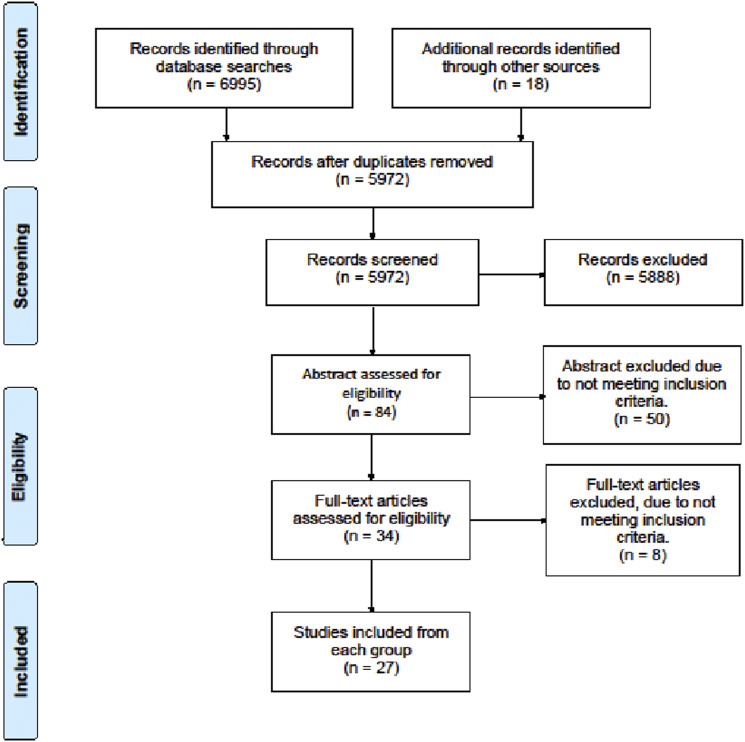
Results: We included 27 studies involving 1886 patients. Nine studies assessed increasing BP during acute reperfusion therapy (intravenous thrombolysis, mechanical thrombectomy, intra-arterial thrombolysis or combined). Eighteen studies tested BP elevation alone. Phenylephrine was the most commonly used agent to increase BP (n = 16 studies), followed by norepinephrine (n = 6), epinephrine (n = 3) and dopamine (n = 2). Because of small patient numbers and study heterogeneity, a meta-analysis was not possible. Overall, BP elevation was feasible in patients with fluctuating or worsening neurological symptoms, large vessel occlusion with labile BP, sustained post-stroke hypotension and ineligible for intravenous thrombolysis or after acute reperfusion therapy. The effects on functional outcomes were largely unknown and close monitoring is advised if such intervention is undertaken.
Conclusion: Although theoretical arguments support increasing BP to improve cerebral blood flow and sustain the ischaemic penumbra in selected AIS patients, the data are limited and results largely inconclusive. Large, randomised controlled trials are needed to identify the optimal BP target, agent, duration of treatment and effects on clinical outcomes.
Keywords: acute; blood pressure; elevation; induced hypertension; ischaemic; stroke; vasopressor.
© European Stroke Organisation 2022.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
-
- CAST . Randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) collaborative group. Lancet 1997; 349: 1641–1649. 1997/06/07. - PubMed
-
- The International Stroke Trial (IST) . A randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. International stroke trial collaborative group. Lancet 1997; 349: 1569–1581. 1997/05/31. - PubMed
-
- Mulder M, Ergezen S, Lingsma HF, et al. Baseline blood pressure effect on the benefit and safety of intra-arterial treatment in mr clean (multicenter randomized clinical trial of endovascular treatment of acute ischemic stroke in the Netherlands). Stroke 2017; 48: 1869–1876. 2017/04/23. DOI: 10.1161/strokeaha.116.016225. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
